RECONSTRUCTIVE APPROACHES
RECONSTRUCTIVE APPROACHES
With a few distinctive caveats, key principles for successful reconstruction of the forehead mimic those of other facial anatomic regions. The forehead is comprised of five cosmetic subunits, including the central forehead, right and left lateral forehead (temples), and right and left eyebrows. While it may be advantageous, or even critical, to confine reconstruction within the boundaries of cosmetic subunits in other areas on the face, there is typically less concern for a repair bridging the cosmetic subunits of the forehead. Instead, reconstructive success is more fundamentally determined by the preservation of forehead subunits in relationship to each other and to the remainder of the facial architecture. Thus, repairs should be designed to maintain the position of the natural hairline and eyebrows, as these landmarks largely define the visual gestalt of the region.
Additionally, there is considerable individual variation in the amount of non–hairbearing skin both inferior and medial to the natural hairline, limiting the size of the central and lateral forehead subunits.2 Proper consideration of this variable is essential, as the location of the hairline determines the size of potential donor tissue reservoirs for
flap repairs and represents an ideal location in which to camouflage incision lines. As with head and neck reconstruction in general, utilization of neighboring tissue, rather than distant skin grafts, is of significant value, as even sizeable flap repairs routinely yield nearly imperceptible scars when appropriately designed and executed.
While the tenet of preserving free margins is inviolable in facial reconstruction, a true free margin—the eyelid—is only occasionally in play when considering forehead defects. That said, the potential to induce lasting eyebrow asymmetry is encountered frequently during reconstructive design. The eyebrows are aesthetically prominent and vulnerable to external tension vectors. Thus, for all intents and purposes, the eyebrows should be considered a free margin, albeit typically a more forgiving one. Thus, it is usually more advantageous to orient a moderately sized primary closure vertically rather than to risk eyebrow elevation with a horizontal approach. Further, there is lower risk for sensory nerve transection with a vertical orientation, and with meticulous suturing technique these scars will typically blend nicely with the surrounding skin.3
Ideally, all repairs should be designed to fall within relaxed skin tension lines (RSTLs), and this precept holds true for reconstruction of the forehead region. RSTLs run in a horizontal arc (perpendicular to the fibers of the frontalis muscle) across the forehead itself, often with a subtle dip at midline where the glabellar musculature pulls overlying skin inferiorly via dermal attachments (Figs. 43-1 and 43-2).
When primary horizontal closure is precluded by the location or orientation of a central forehead wound, the glabellar furrows may provide a strategic location in which to hide a vertically oriented curvilinear incision. At approximately the temporal line, the RSTLs begin to curve inferiorly, and in most patients become accompanied by the periocular rhytides, thus allowing incision lines to be thoughtfully placed in a number of orientations. For modestly sized defects located anteriorly on the temple, horizontal repair within the periocular rhytides is often effective, while similar defects located laterally are typically best repaired with incision lines positioned parallel to the natural hairline (Fig. 43-3).
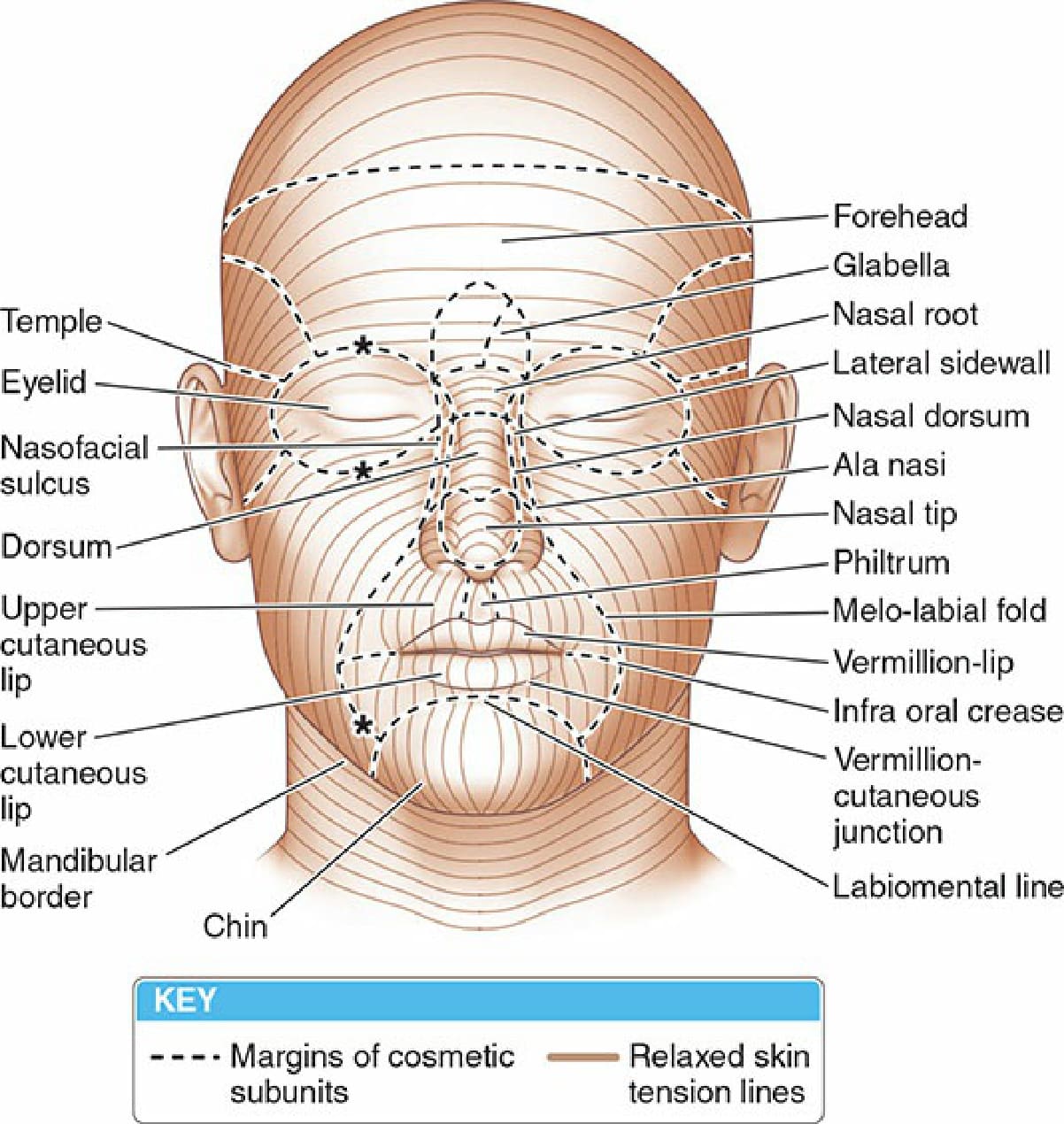
Figure 43-1. The relaxed skin tension lines of the face tend to run perpendicular to the mimetic musculature, with a slight downward pull induced by a gravitational vector.

Figure 43-2. (A) This preoperative photograph illustrates the subtle downward arc often present at midline as the otherwise horizontally oriented RSTLs traverse the central forehead. (B) The defect was horizontally oriented after tumor extirpation. (C) The primary closure was gently curved to fall along this patient’s RSTLs. (D) At follow-up, brow position is maintained and incision lines are nicely camouflaged.

Figure 43-3. (A) While the anterior limb of a horizontally oriented repair could be hidden by this patient’s periocular rhytides, a better design choice positions incision lines to fall along the hairline. (B) There is no pull on the lateral canthus at immediate repair. (C) At 3 month follow-up, the incision line is nearly imperceptible.