Flaps — Part 2
The triangular shape of the distal flap does not correspond to most circular defects. The surgeon can either trim the flap to match the defect or enlarge the defect to accommodate the flap. Since the distal flap has the most tenuous blood supply, it is usually preferable to trim the excess tissue of the flap to match the defect. For a full discussion of transposition flaps, see Chapter 23.
Bilobed flap. If a rhombic flap is not possible because tension on the skin immediately adjacent to the primary defect is excessive or causes anatomic distortion, the bilobed flap can reach suitable donor sites more remote from the defect (Fig. 42- 26). Compared to the rhombic flap, the geometry and execution of the bilobed flap are more complex.26–29
Like the rhombic flap, the bilobed flap also rotates approximately 90 degrees. However, the bilobed flap distributes the rotation between the two lobes, each rotating 45 degrees. The second lobe adds a z-plasty that helps to push the flap toward the primary defect. The tension vector to close the donor site for the secondary lobe (i.e., the tertiary defect) should not pull on the nearby free margins.
The first key suture closes the tertiary defect and pushes the flap toward the primary defect. The second key suture sets the primary lobe into the defect. The exact position of this suture may vary or require adjustment to create tension vectors that avoid anatomic distortion, to align the standing cone, and to adjust the sizing of the primary lobe. It is often preferable to ensure that closure of the standing cone deformity preserves contour before trimming excess tissue for a precise fit. The secondary lobe will generally have excess length and require trimming to match the secondary defect. For a full discussion of bilobed flaps, see Chapter 24.
Trilobed flap. The trilobed flap has tissue mechanics similar to the bilobed flap with a few distinct advantages (Fig. 42-27). First, its third lobe allows the flap to reach tissue reservoirs increasingly remote from the primary defect, and it is particularly useful to reconstruct large cheek defects. Second, the third lobe extends the arc of rotation to 120 to 150 degrees and may provide a more favorable tension vector to close the quaternary defect. Third, the additional lobe adds the benefit of another zplasty, which decreases the tension to transpose the flap, an important advantage when even mild tension at the distal flap can distort the free margins. Finally, the third lobe increases the width of the flap pedicle. If the orientation of the standing cone would cut into the pedicle of a bilobed flap, the increased pedicle size of a trilobed flap can
improve blood supply.30
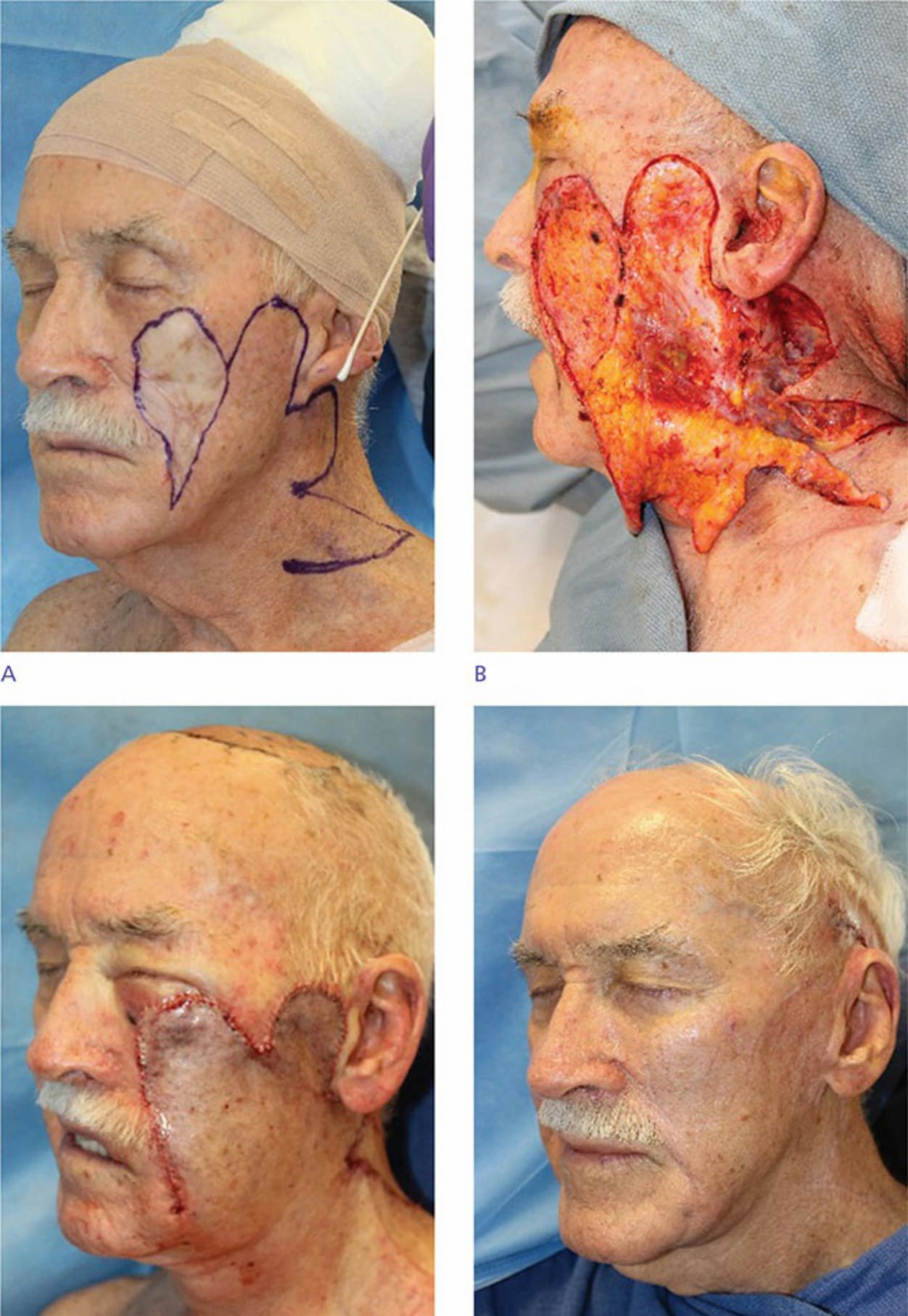
Figure 42-27. (A) A trilobed flap is designed to replace this large skin graft. (B) Intraoperative photo demonstrating the degree of flap elevation. Appearance immediately postoperatively (C) and at follow-up (D).