Flaps
Flaps
Advancement flaps Advancement flaps rely on a random-pattern blood supply and are useful for wounds that could be closed with a fusiform closure, but one of the standing cones falls in an unfavorable position. An advancement flap maintains tension along the same single vector as a fusiform closure, but it displaces the undesirable standing cone to a more favorable position. In contrast to rotation flaps, advancement flaps do not create secondary defects. Infraorbital wounds in zone 1 and large preauricular wounds in zone 2 are the most common indications for advancement flaps on the cheek.
Zone 1 wounds on the medial infraorbital cheek and nasofacial sulcus often require advancement flaps to deviate the superior standing cone away from the lower eyelid margin (Fig. 42-17). A standing cone is excised from the inferior aspect of the wound. A horizontal incision is made from the superior aspect of the wound laterally toward the temple, and the superior standing cone is shifted laterally toward the crow’s feet or sutured out using the rule of halves. Ideally, the horizontal incision is concealed in the cosmetic subunit junction line between the cheek and lower preseptal eyelid. If the superior aspect of the wound does not abut this boundary, the primary defect may be extended superiorly to avoid creating a noticeable horizontal scar in the middle of the cheek subunit. The flap is undermined and advanced from lateral to medial. The zygomatic ligament may restrict medial advancement, and an unanticipated secondary defect can result along the orbital rim if the flap is stretched too aggressively. For this reason, a pure advancement flap is indicated only for small defects. To avoid ectropion from a secondary defect along the orbital rim, it may be necessary to convert to a rotation flap by extending the lateral incision in an arc to the temple and preauricular area.
Vertically oriented fusiform closure of larger wounds in the preauricular area of zone 3 is frequently not possible because of excessive tension. If a horizontally oriented fusiform excision would be possible, but the auricular cartilage obstructs the posterior standing cone, an advancement flap that slides skin superiorly from the lower cheek and neck may be designed (Fig. 42-18). A horizontally or tangentially oriented standing cone is excised from the anterior aspect of the primary defect. A vertical incision is made from the lateral wound toward the neck, and the posterior standing cone is displaced inferiorly to tuck under the earlobe. Ideally, the vertical incision is camouflaged in the preauricular crease. If the posterior aspect of the wound does not abut this boundary, the primary defect may be extended posteriorly to avoid making a noticeable vertical scar in the middle of the cheek subunit. The flap is undermined and advanced from inferior to superior. For a full discussion of advancement flaps, see Chapter 21.
Rotation flaps Rotation flaps have a random pattern blood supply and distribute tension across multiple vectors to minimize distortion at the primary defect. The hallmark of a rotation flap is the arciform incision used to mobilize the surrounding skin. Rotating the flap into the primary defect creates a secondary defect along the arciform incision. A greater arc of flap rotation increases the size of the secondary defect. Tension is distributed along multiple vectors at both the primary and secondary defects.
The cervicofacial rotation flap is used to close larger defects in zone 1 of the anterior cheek (Fig. 42-19). A standing cone is excised along the inferior border to the defect. An arciform incision is made from the lateral defect toward the temple. It is important to extend the incision superior to the lateral canthal angle, as the increased height of the flap will help prevent a secondary defect along the lower preseptal eyelid
margin. Depending on the size of the wound or tension on the flap, the arciform incision may be extended posteriorly along the sideburn, preauricular crease, and neck. Smaller, lower tension wounds usually do not require such a large arc to the flap.
after surgery. Note removal of the standing cone along the outer edge of the arc (black arrowhead). (D) The scar is minimally apparent at follow-up.
The flap is elevated. Sharp undermining is necessary to release the zygomatic ligament and mobilize the flap. The flap is rotated medially toward the defect. Care is taken to keep the main tension vectors parallel to the lower eyelid margin. Despite wide undermining, tension may still be too great for primary closure. A backcut of the flap with or without a z-plasty may facilitate closure (Fig. 42-20).
Even with proper design, a secondary defect at the infraorbital cheek may still threaten ectropion. To close this gap, the flap can slide toward the defect with a combination of rotation and superomedial advancement. If the surgeon anticipates the
possibility of superomedial advancement, it is best not to excise the inferior standing cone until the flap is set and the preferred location of the standing cone is obvious. Tacking the undersurface of the flap to the inferior orbital rim is often helpful to transfer tension to the immobile bone and decrease tension of the dermal sutures at the flap edges. Asking the patient to open his or her eyes and mouth and look up is the most effective way to assess the position of the lower eyelid.
After setting the flap in the primary defect, the secondary defect along the arciform incision is closed. In general, the edge of the flap is hiked superiorly toward the temple or superolaterally toward the ear. Tacking the undersurface of the flap to the zygomatic ligament or the lateral orbital rim may be necessary to transfer tension away from the eyelid. If the flap was rotated toward the primary defect along a substantial arc, then direct closure of the secondary defect may not be possible. Second intention healing or skin grafting may be necessary when closure of the secondary defect is not possible.
In patients with a generous reservoir of skin in the nasolabial fold or jowl, it may occasionally be preferable to design an inferiorly based rotation flap (Fig. 42-21). This design is best suited for zone 1 defects that have their greatest diameter in the horizontal dimension. A standing cone is excised laterally toward the temple. An arciform incision extends from the medial aspect of the primary wound inferiorly along the nasofacial sulcus and nasolabial fold. The flap is elevated and rotated from inferior to superior. The secondary defect along the nasofacial sulcus and nasolabial fold is closed. This flap design must be used cautiously, because the vertically oriented tension vector at the primary defect has a high risk for ectropion, and direct closure of a large secondary defect along the arciform incision can pull the nose laterally. To minimize tension at the eyelid, it is almost always necessary to tack the leading edge of the flap to bone at the infraorbital rim. For a full discussion of rotation flaps, see Chapter 22.
fold (black arrowhead). (C) The position of the eyelid is undisturbed immediately postoperatively. (D) The scar is minimally apparent at follow-up and eyelid position is intact.
V-Y Island pedicle flaps V-Y flaps are a common option to reconstruct medium- to large-sized defects of the cheek. They differ from other sliding flaps (e.g., advancement and rotation) in two ways. First, their entire blood supply comes from the flap’s undersurface since the dermis is incised around the entire periphery. Second, they are not simply stretched toward the defect, but also pushed toward the primary defect by closure of the secondary defect. Zones 1 and 3 are the most common cheek locations where V-Y flaps are employed. The superficial fat pads beneath the skin in these locations are highly mobile and typically allow the flap to be advanced greater distances than in zone 2.
Traditional V-Y island pedicle flaps are inferiorly based and triangular in design (Fig. 42-22). Flap limbs originate from the medial and lateral caudal borders of the defect and extend inferiorly toward to the mandible. Zone 2 V-Y flaps are most mobile when incisions are carried past the mandible into the jowl and neck area. An angle less than or equal to 30 degrees should be created where the flap limbs meet. Depending upon the size and location of the defect, one or both of the flap limbs may be hidden in a cosmetic junction border such as the melolabial fold or preauricular crease.
The V-Y flap is circumferentially incised to the level of the SMAS and the peripheral edges are undermined in this plane. The central 30% to 50% of the subcutaneous tissue is preserved, and it is this pedicle upon which the flap “rocks” forward in a superomedial vector. Once careful hemostasis has been achieved, the flap is sutured in
place. The risk of ectropion for zone 1 defects can be minimized by tacking the leading edge of the flap to the infraorbital rim.25
The conventional design of the V-Y advancement flap has a number of limitations. First, fascial attachments restrict superior advancement of the flap and may result in undesirable pincushioning. Second, the horizontal scar of the flap’s leading edge is often conspicuous. Finally, traditional V-Y flaps may not stretch to cover tall defects.
Wide undermining of the peripheral skin may help minimize the trapdoor effect of the triangular flap. A crescentic design modification addresses the horizontal scar when employed for defects in the medial portion of zones 1 and 3. Rather than incising the flap at the lateral and medial defect borders, the flap’s leading edges are designed off of the cephalic and caudal defect borders. These limbs then curve around to follow the relaxed skin tension lines of the cheek. As the flap moves superomedially, the leading edge is sutured to align with the cosmetic junction border (Fig. 42-23). A “pac-man” design modification gains length by rotating the leading edges of the flap to the distal defect (Fig. 42-24). The final flap scar is fusiform with a line through the center where the two arms meet. If there is concern for vascular compromise, the redundant cone at the flap’s midpoint can be removed at a later date. Frequently, slight tissue protrusions in this location self-resolve. For a full discussion of V-Y island pedicle flaps, see Chapter 25.
Transposition flaps Transposition flaps avoid distortion at the primary defect by displacing key tension to the adjacent tissue reservoirs and by reorienting tension to more favorable vectors. On the cheek, transposition flaps are especially useful for large defects in zones 1 and 3 when tension at the primary defect from a linear closure or sliding flap would distort the position of the mouth, nose, or eyelid.
As opposed to sliding flaps, which have the greatest tension at the primary defect, transposition flaps displace the greatest tension to the final donor site (i.e., secondary defect of a rhombic flap; tertiary defect of a bilobed flap; and quaternary defect of a trilobed flap). By transferring tension to the donor defects, the transposition flap can be rotated to the primary defect with minimal tension. Transposition flaps for upper cheek defects recruit from the looser skin on the lower half of the cheek; and those for lower cheek defects recruit from the lax skin on the neck.
Rhombic transposition flaps. The rhombic flap is a workhorse flap for many cheek defects. The flap extends from the midline of the defect toward the desired tissue reservoir. For cheek defects, the open limb of the flap usually points to the jowl or neck. The classic rhombic flap has a 60-degree angle at its apex, but lengthening the flap to create a more acute apical angle can facilitate closure and avoid a standing cone deformity at the donor site (Fig. 42-25).
To avoid secondary motion at the primary defect, the flap should have approximately the same surface area as the primary defect and extend perpendicularly from the primary defect. The first key suture closes the secondary defect and bears the greatest amount of tension. The second key suture sets the flap into the primary defect and determines its arc of rotation as well as the position of the standing cone. As the arc of rotation increases, pivotal restraint effectively shortens the flap, making it more difficult for its distal edge to reach the defect, and the standing cone deformity may encroach on the flap pedicle. It is preferable to set the flap so that the standing cone deformity does not narrow the pedicle Removing the standing cone is often reserved until the flap has been set in its ideal location.

Figure 42-17. (A) Both a primary closure and advancement flap were considered with this infraorbital cheek defect. (B) An advancement flap was performed to avoid encroachment of the superior standing cone on the lower eyelid. (C) The patient has a minimally apparent scar and preserved eyelid position at follow-up.

Figure 42-18. (A) Rhombic and advancement flaps were considered for this preauricular cheek defect. (B) An advancement flap was performed. An incision was made along the preauricular crease, and the posterior standing cone was displaced behind the earlobe. (C) The scar is minimally apparent at follow-up.
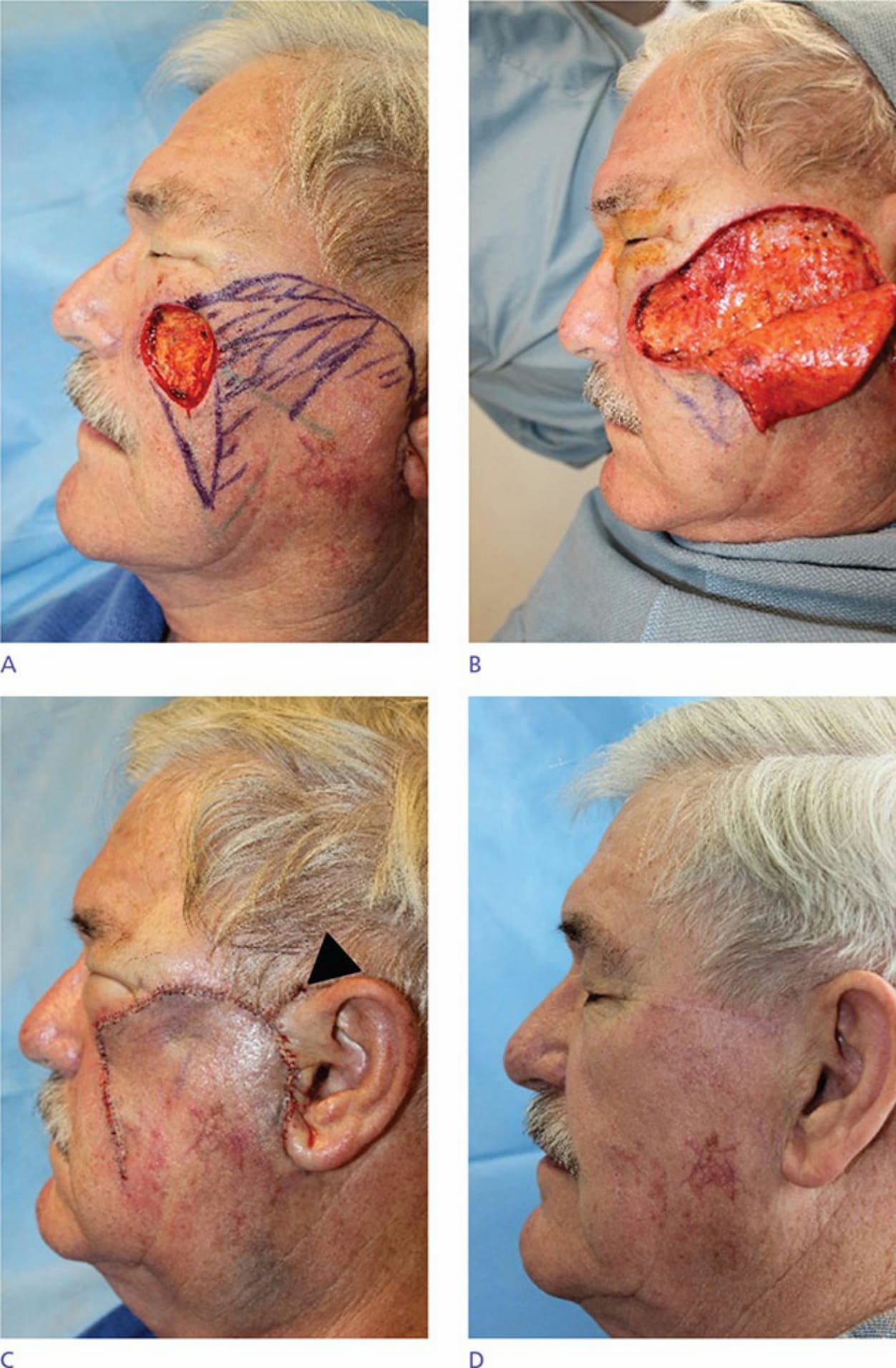
Figure 42-19. (A) Rotation flap is designed for a defect of the medial zygoma. Note that the incision line was extended superior to the lateral canthal angle to prevent a secondary defect along the lower preseptal eyelid margin. (B) Intraoperative photo demonstrating the arciform incision and extent of undermining. (C) Appearance immediately

Figure 42-20. Example of a rotation flap with a backcut and z-plasty to improve mobility.

Figure 42-21. (A) An inferiorly based rotation flap is designed for this infraorbital cheek defect. (B) Intraoperative photos illustrating the vertical tension vector on the primary defect (black arrow). Tacking the leading edge of the flap to the bone at the infraorbital rim decreases tension on the lower eyelid. Note the secondary defect at the nasolabial
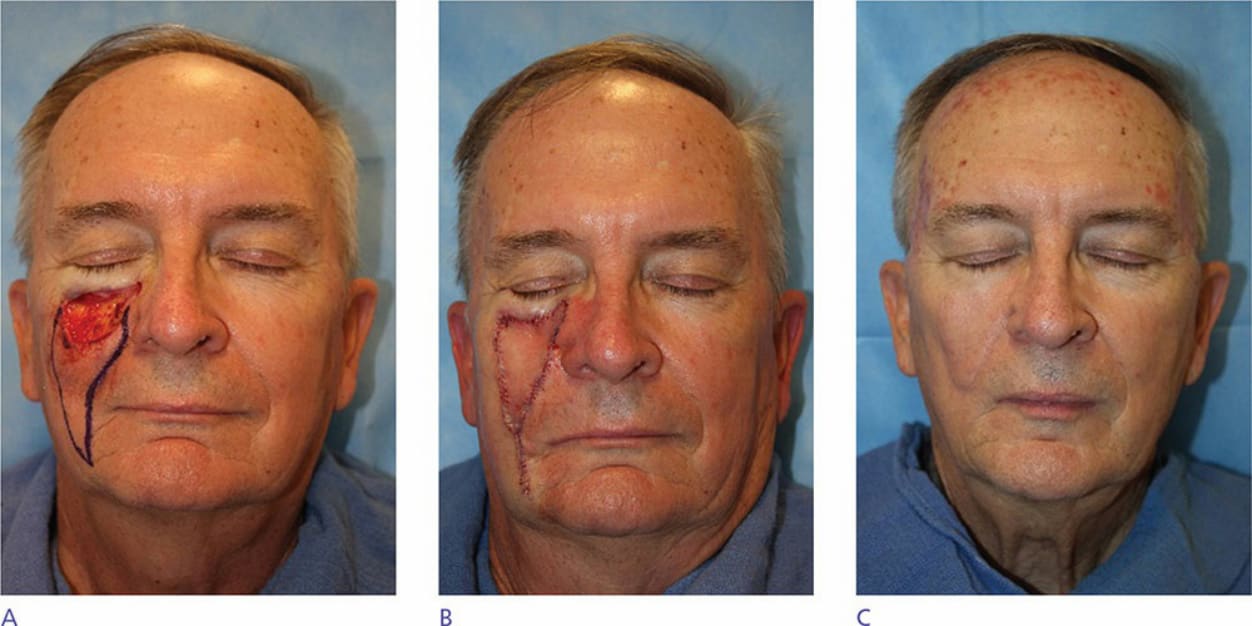
Figure 42-22. (A) A traditional V-Y island pedicle advancement flap is designed for this infraorbital cheek defect. (B) The leading edge of the flap has been tacked to the infraorbital rim to avoid downward pull on the eyelid. (C) Eyelid position is intact and much of the scar hides in cosmetic subunit junction lines.

Figure 42-23. (A) A crecentic V-Y island pedicle advancement flap has been designed for this medial cheek defect. Note that the lateral arm of the flap originates from the distal (i.e., superior) defect. (B) Appearance immediately postoperatively. (C) Scar at short-term follow-up.

Figure 42-24. (A) A “pac-man” V-Y island pedicle advancement flap has been designed for this defect. Note that the flap limbs originate from the distal defect to gain reach. (B) Appearance immediately postoperatively. Removal of the central standing cone was delayed for several weeks to preserve blood supply. (C) Minimally apparent scar at follow-up.
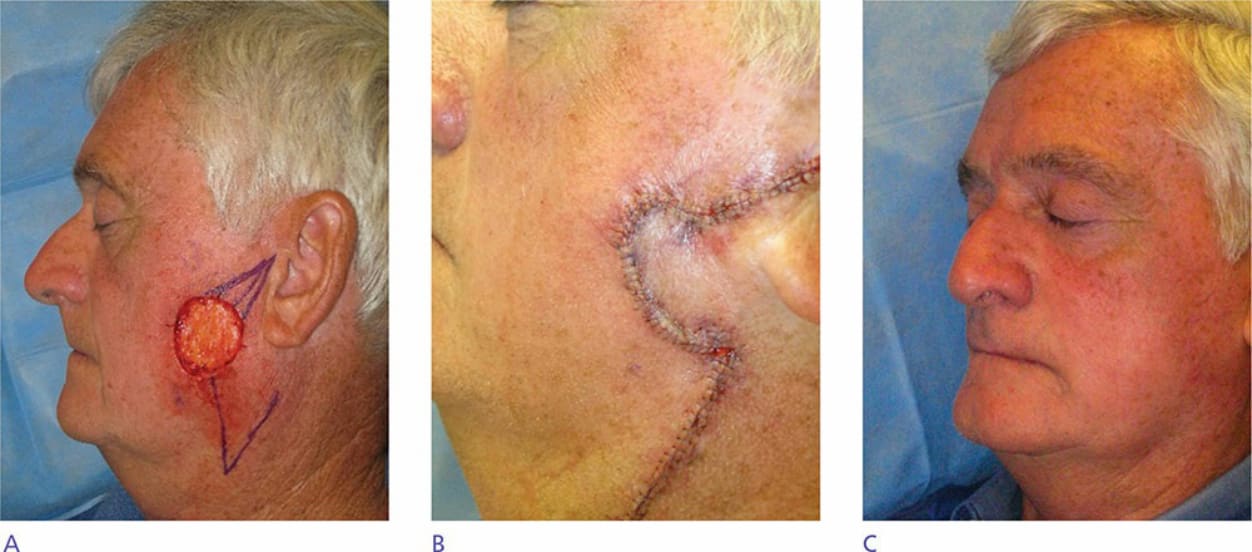
Figure 42-25. (A) A rhombic flap is designed to reconstruct this lower cheek defect. Note that the open limb of the flap points to the tissue reservoir on the neck. Appearance immediately postoperatively (B) and at follow-up (C).

Figure 42-26. (A) A bilobed and trilobed flap was considered and designed for this large medial cheek defect. The trilobed flap design was not necessary. (B) Appearance immediately postoperatively. (C) Scar is inconspicuous at follow-up.