Primary closure
Primary closure
Primary closure with side-to-side approximation of the edges of a fusiform wound is the most common reconstruction method for cheek defects.24 Tension lies along a single
vector running perpendicular to the long axis of the fusiform design, and is greatest at the center and decreases toward the apices. Linear closures are usually oriented parallel to the relaxed skin tension lines, which the patient can accentuate with a forceful smile. To avoid standing cones and to maintain normal contour, the ideal angles at the apices of a fusiform excision are <30 degrees, which requires a length:width ratio of at least 3:1. The ideal orientation of fusiform closures on the cheek depends on wound location.
Fusiform closures of zone 1 wounds are usually oriented with the long axis perpendicular to the lower eyelid (Fig. 42-9). The horizontal tension vector from this design prevents lower lid ectropion. Elongation of the central axis after wound closure may temporarily push up on the lower eyelid, which usually returns to normal position within a couple of weeks. An M-plasty may be used to keep the superior standing cone from encroaching on the lower eyelid margin. For infraorbital cheek defects that have a longer horizontal diameter, an S-plasty may be used to keep tension vectors parallel to the free eyelid margin (Fig. 42-10).
Linear closures in zone 3 are generally designed with the long axis parallel to the nasolabial fold and parallel to the relaxed skin tension lines (Fig. 42-11). Fusiform closures predictably flatten the nasolabial fold and can pull on the free margin of the lips and oral commissure. The wound can bow with central depression and relative
elevation toward to apices. If the asymmetry from the flattened nasolabial fold or bowed scar is noticeable or if the free margin distortion is greater than can be expected to resolve over time, a local transposition flap may be preferred (Fig. 42-12). A crescentic design with the longer posterior curve is a variation of the fusiform excision that may be used to create a curvilinear scar mimicking the relaxed skin tension lines (Fig. 42-13).
The orientation of linear closures varies between the superior and inferior regions of zone 2. Fusiform closures near the zygomatic arch are often oriented along a tangent continuous with the crow’s feet (Fig. 42-14). Wounds closer to the mandible are usually repaired with a vertically oriented axis. Tension increases for wounds closer to the preauricular sulcus, because the auricular cartilage restricts advancement of the posterior wound edge. To avoid excessive tension, advancement or transposition flaps may be preferred for larger preauricular wounds. For a full discussion of linear closures, see Chapter 18.
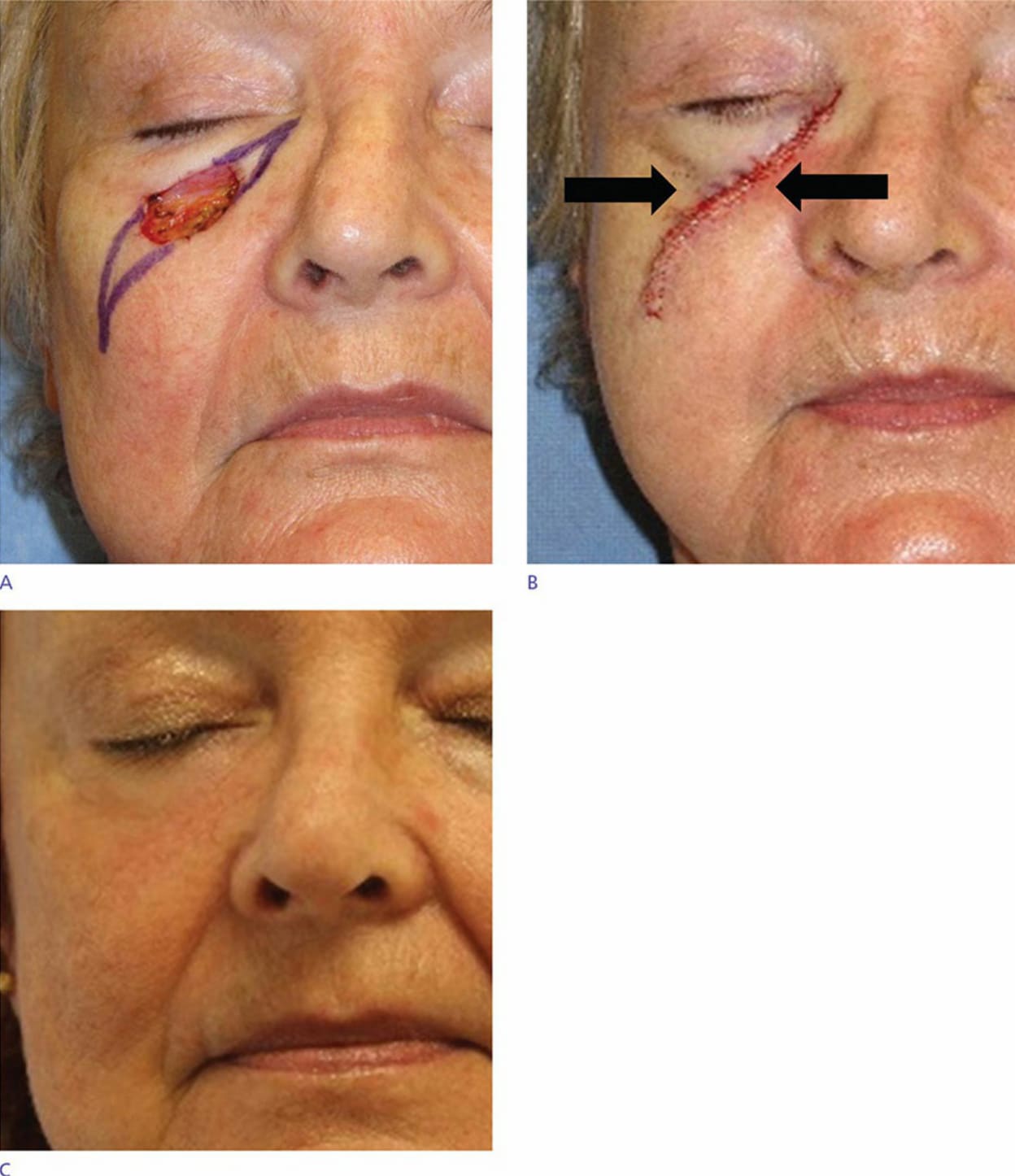
Figure 42-9. (A) A primary closure with a long axis perpendicular to the eyelid is designed for this zone 1 cheek defect. (B) The horizontal tension vector (black arrows) avoids ectropion. (C) Eyelid position is preserved and the scar is minimally apparent at follow-up.
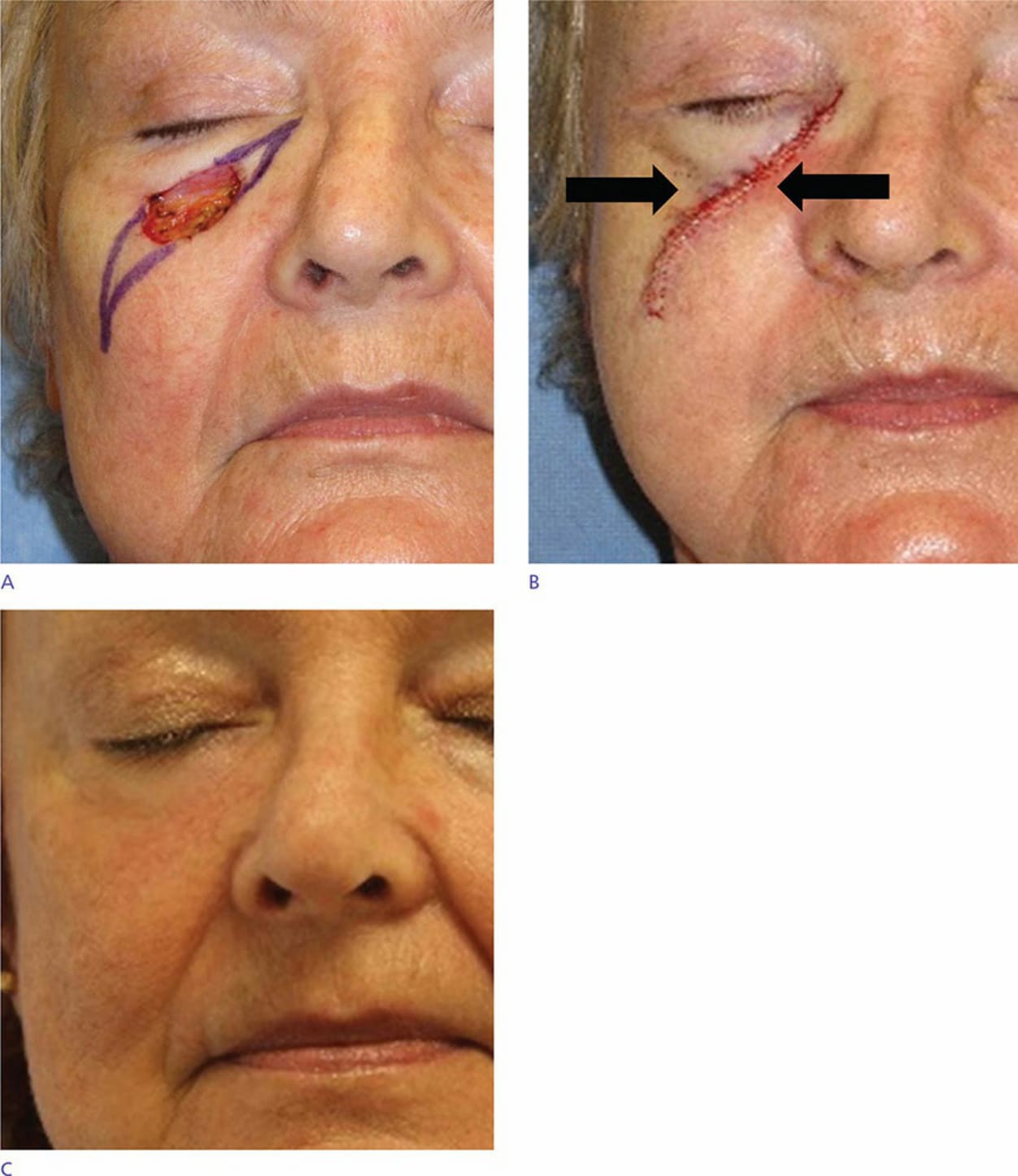
Figure 42-10. (A) An S-plasty is designed for this infraorbital cheek defect with a long horizontal axis. (B) The horizontal tension vectors of the S-plasty avoid ectropion. (C) Eyelid position is preserved and the scar is minimally apparent at follow-up.
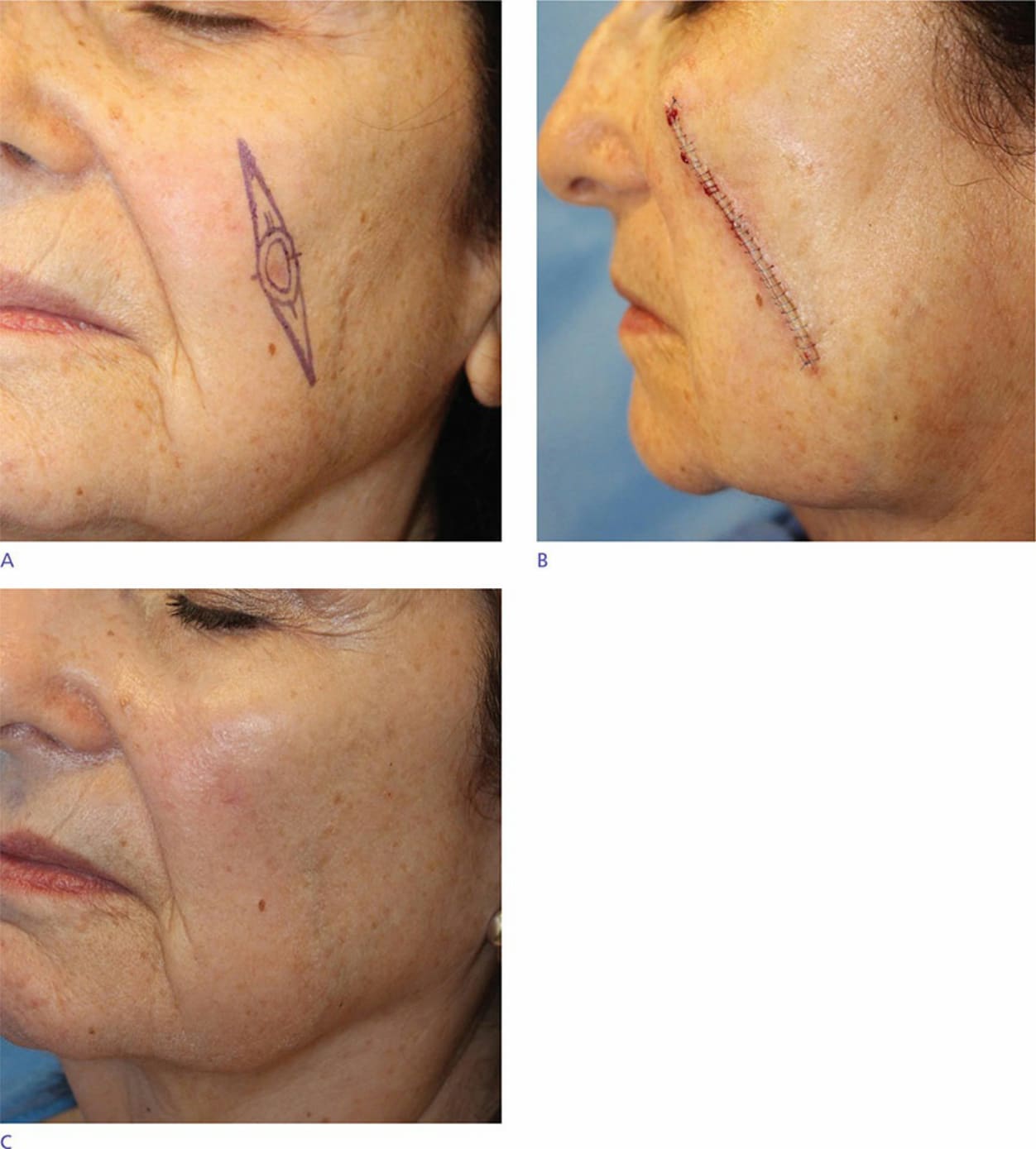
Figure 42-11. (A) A fusiform excision parallel to the nasolabial fold is designed for this zone 3 cheek lesion. (B) The sutured wound falls within relaxed skin tension lines. (C) The scar is minimally apparent and the nasolabial fold has retained volume at follow-up.

Figure 42-12. Tight zone 3 closures can flatten the nasolabial fold. (A) A rhombic flap and primary closure were considered for this zone 3 defect. (B) The wound was repaired with a primary closure. (C) Flattening of the nasolabial fold from wound tension reveals central facial asymmetry at follow-up.

Figure 42-13. Crescentic fusiform excision. (A) A crescentic design was employed to create a curvilinear scar mimicking the relaxed skin tension lines. (B) Sutured wound immediately postoperatively. (C) Imperceptible scar along the relaxed skin tension line at follow-up.

Figure 42-14. (A) A tangential fusiform closure is designed to parallel the crow’s feet. (B) Eyelid position is preserved despite wound tension. (C) The scar is minimally apparent at follow-up.