ANATOMY
ANATOMY
Medially, the cheek joins the nose at the nasofacial sulcus, the lips at the melolabial fold, and the chin at marionette lines. Inferiorly, the cheek extends to the mandible. Laterally, it extends to the ear. Superiorly, the orbital rim and the zygomatic arch delineate the cheek from the eyelid and temple. This section will focus on key anatomic principles to consider for cheek reconstruction.
The cheek covers and protects the facial nerve branches and parotid duct
The skin of the cheek covers and protects the branches of the facial nerve and the parotid duct. The parotid gland lies over the masseter muscle, and its parenchyma adds extra protection to the facial nerve on the posterior one-third of the cheek. The branches of the facial nerve and parotid duct are most vulnerable after they emerge from the parotid gland and course through the anterior cheek. The superficial musculoaponeurotic system (SMAS), which is continuous with the platysma inferiorly and the superficial
temporal fascia superiorly, protects all of the branches of the facial nerve and parotid duct.1
Topographic landmarks help map the paths of the facial nerve branches that course through the cheek.2 The frontal branch follows a line from 0.5 cm below the tragus to 1.5 cm above the lateral brow (Fig. 42-1). Its rami cross over the periosteum of the zygomatic arch before traversing the temple on their way to innervate the frontalis, orbicularis oculi, corrugator supercilii and anterior and superior auricular muscles. The zygomatic and buccal branches have numerous communications as they cross the anterior two-thirds of the cheek to innervate the lip elevators and nasal muscles. The midway point on a line drawn from the root of the helix to the lateral commissure of the mouth identifies the path of the branch that innervates the zygomaticus major muscle.3 The marginal mandibular nerve courses along the inferior border of the mandible and crosses immediately superficial to the facial artery at the anterior border of the masseter muscle before supplying the lip depressor muscles (Fig. 42-2).
The parotid duct emerges from the anterior border of the parotid gland approximately 1 cm inferior to the zygomatic arch. It runs in an anterior direction superficial to the masseter muscle and deep to the buccal branch of the facial nerve (Fig. 42-3).4 The transverse facial artery accompanies the duct. At the anterior border of the masseter muscle, the duct dives medially, pierces the buccinator muscle, and drains saliva into the oral cavity at the parotid papilla opposite the second upper molar.
The contours of the cheek reflect the shape of the underlying fat pads. These contours change with age
A thin layer of tightly organized fat is firmly attached to the dermis of the cheek skin. For most local reconstructions of the cheek, the undermining plane lies immediately deep to this subdermal layer of fat and above the superficial fat compartments. Compared to the compact subdermal fat, the underlying superficial fat compartments have grossly larger and more loosely organized fat lobules (Fig. 42-4). Fibrous septae divide the superficial fat into distinct anatomic zones, including the nasolabial, medial, middle, lateral, and jowl compartments.5,6 These fibrous septae correspond to the location of some of the retaining ligaments of the face (Fig. 42-4C).7 The deep fat compartments, including the medial, lateral, and buccal fat, comprise a third layer that buttresses the superficial fat and adds to cheek projection.5,8
These superficial and deep fat compartments alter the volume and projection of the cheek during the aging process. The angular or inverted triangular appearance of the youthful face results from the juxtaposition of the concave buccal cheek and the convex, fat-filled malar and lateral cheek.9 Descent of the superficial fat pads of the cheek contributes to the square configuration of the aged face.9 The fat pads are also important during reconstruction. Undermining that includes the deeper layers of fat may impart a bulky appearance, and mobility may improve when the flap pedicle is centered over the relatively pliable fat compartments.
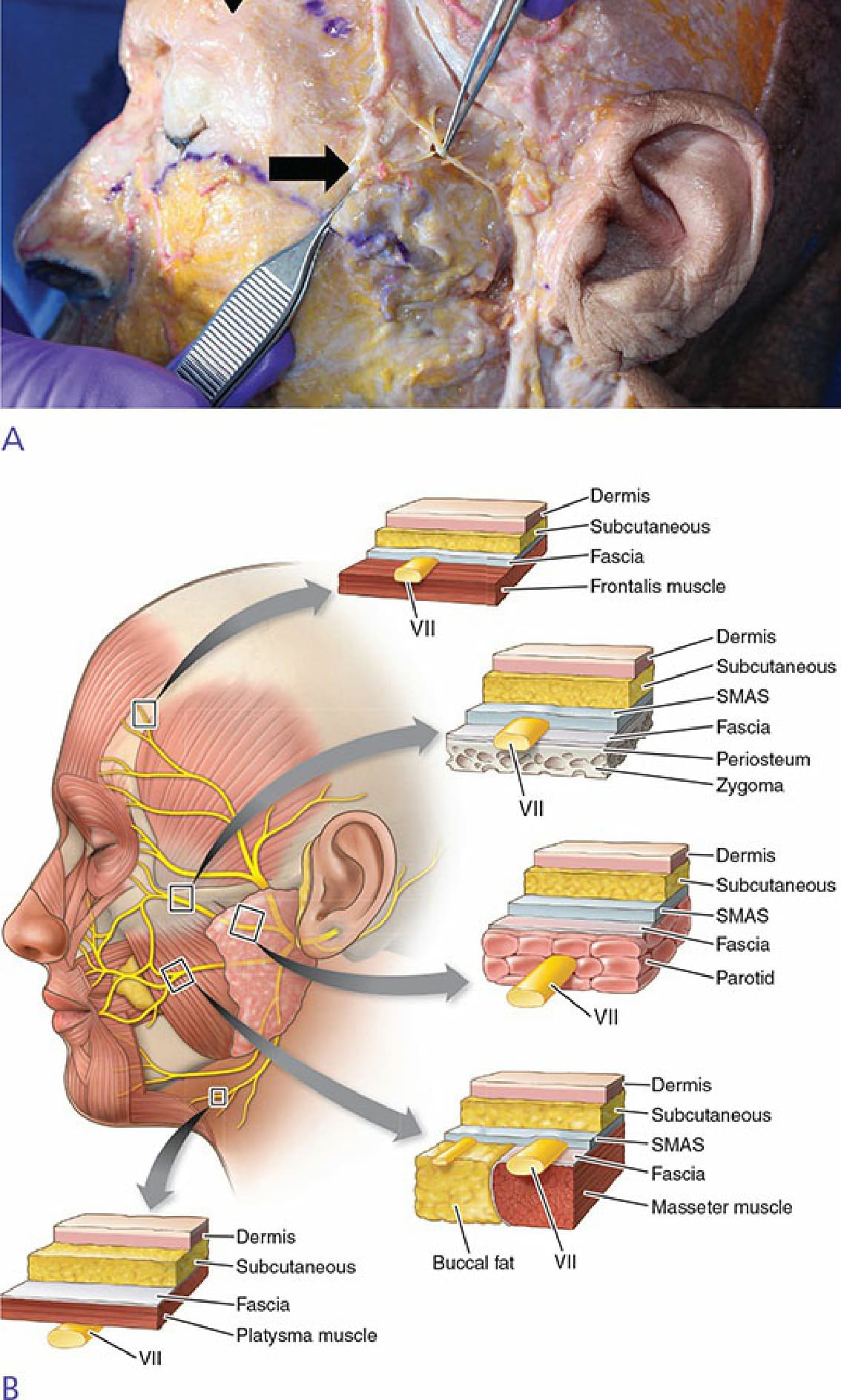
Figure 42-1. Temporal nerve anatomy. (A) The course of the temporal branch was mapped topographically from 0.5 cm below the tragus to 1.5 cm superior to the lateral brow (arrowhead indicates anticipated path of the nerve). The superficial musculoaponeurotic system has been incised and retracted (black arrow), revealing the main ramus of the temporal branch of the facial nerve. (B) Differential depth of the facial nerve.
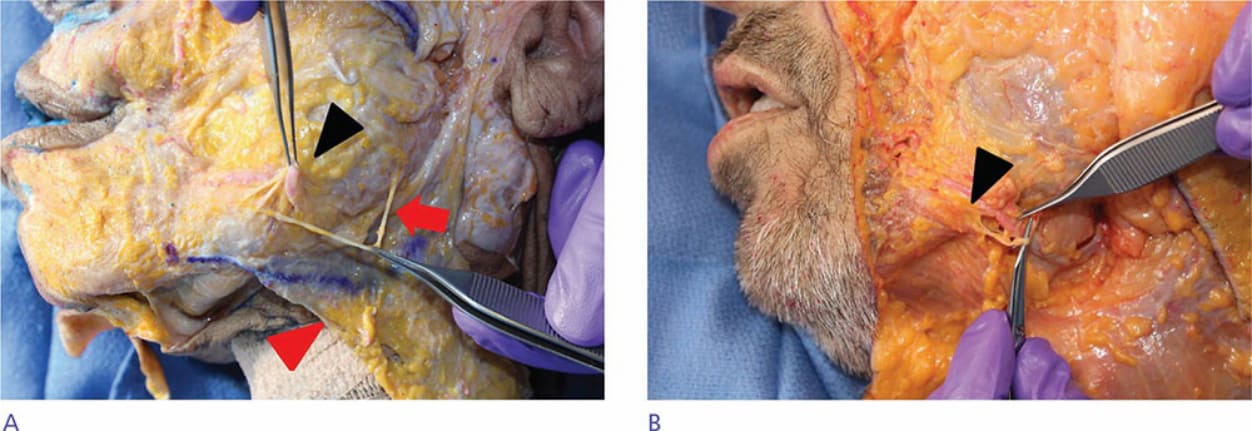
Figure 42-2. Marginal mandibular branch of facial nerve. (A) The SMAS has been retracted (red arrowhead) and the marginal mandibular nerve (red arrow) has been dissected as it courses from the tail of the parotid gland along the mandible to the lip depressor muscles. Note that the nerve passes superficial to the facial artery (black arrowhead). (B) Another cadaver dissection demonstrating innervation of the depressor anguli oris by the marginal mandibular nerve (black arrowhead).
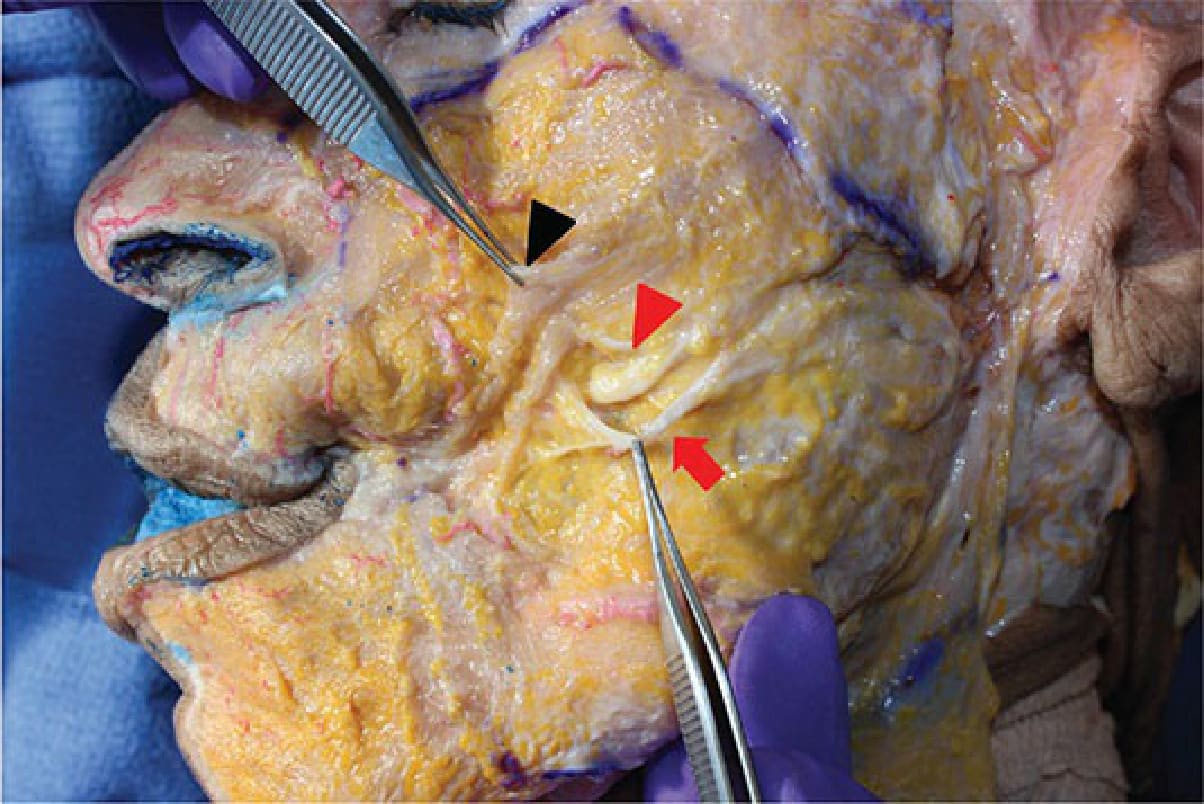
Figure 42-3. Anatomy of the parotid duct. The SMAS has been incised and elevated (black arrowhead). The buccal branch of the facial nerve (red arrow) courses parallel and superficial to the parotid duct (red arrowhead), which is seen here as it dives medially at the anterior border of the masseter muscle to pierce the buccinator muscle and empty into the mouth.
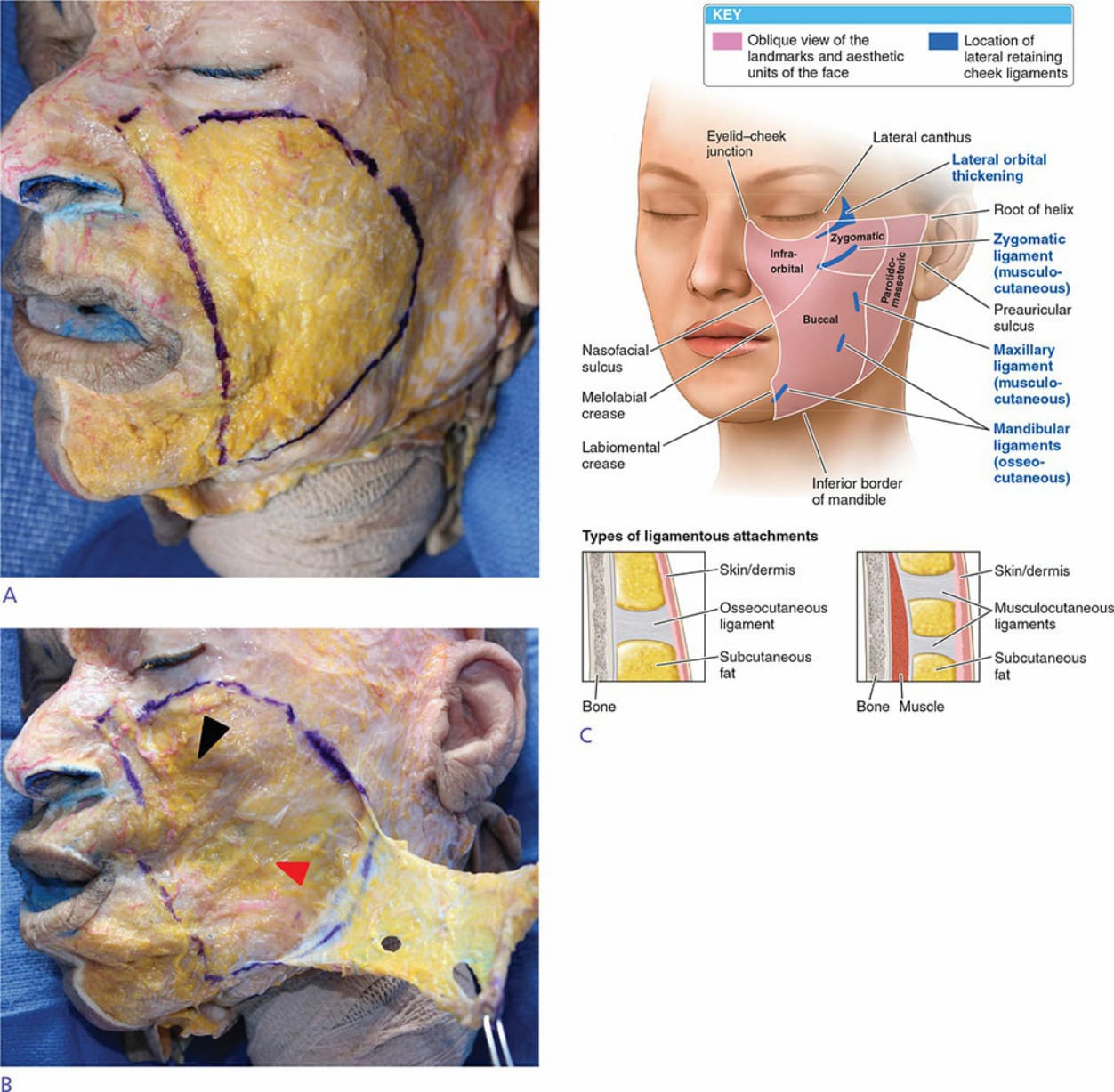
Figure 42-4. Anatomy of fat pads of the cheek. (A) The skin and the subdermal layer of fat have been removed, revealing the underlying superficial fat pads (outlined in purple ink). These fat lobules are larger and disorganized, relative to the smaller, tightly organized subdermal fat. (B) The superficial fat pads have been retracted revealing the deep medial (black arrowhead) and buccal fat pads (red arrowhead). Note that the retracted superficial fat pads are contiguous with the SMAS of the platysma and superficial temporal fascia. (C) The retaining ligaments of the cheek.