Postauricular interpolation flap
Postauricular interpolation flap
The PIF is an ideal reconstructive option for ear defects that are too large for local flaps or need more structural support or volume than skin grafts. The PIF is ideally for tall defects or composite defects near the free margin of the pinna. The PIF may be combined with free cartilage grafts to add contour and support.
A template of the defect is transferred to the skin of the postauricular sulcus and mastoid. The position of the template is modified, depending on the size and characteristics of the primary defect. For defects isolated to the helical rim, the leading edge of the flap can be drawn directly within the postauricular sulcus. As the template is drawn toward the mastoid skin, these horizontal lines may be widened slightly and Burow’s advancement triangles may be added to facilitate additional flap movement. For defects that extend on the antihelix, the PIF will gain additional length by locating the leading edge of the flap on the postauricular skin (Fig. 41-24). An isthmus of posterior auricular skin between the leading edge of the flap and the proximal defect is left to prevent scarring between the raw surfaces of the posterior auricular cartilage and mastoid. Ideally, the base of the PIF will not include hair that could be transferred to the ear.
Cartilage grafts should be considered if the structural integrity of the ear or convex silhouette of the helical rim has been compromised. Conchal bowl cartilage of the contralateral ear can be used as a C-shaped strut under the PIF for larger, full-thickness helical rim defects (Fig. 41-25). The graft may be sutured to the edges of the defect before transferring the PIF.
The anterior and lateral edges of the PIF are incised to the perichondrium (if the leading edge of the flap is designed on the postauricular surface) and mastoid fascia. The flap is elevated at the level of the perichondrium to the posterior sulcus, where it transitions to mastoid fascia. The dissection is carried as far proximally as necessary in order to have the flap comfortably reach the most distal aspect of the surgical defect. If necessary, superior and inferior Burow’s triangles may be removed at the proximal base of the PIF, which can assist flap movement toward the distal aspect of the defect.
Careful hemostasis is necessary, since the donor site will not be accessible once the flap is transferred to the ear. If tension is excessive, the pinna may be pinned to the mastoid with sutures to help the flap reach the defect more easily. The PIF key sutures align the leading edge of the flap to the recipient area. Buried vertical mattress sutures at the helical rim attachments evert tissue to maintain the natural convexity. If the PIF extends over the scaphoid fossa, quilting sutures may be used to tack the flap down in this area and attempt to recreate the natural concavity.34
Takedown is performed approximately 2 to 4 weeks after the initial procedure when the flap pedicle is divided at its proximal base near the mastoid hairline. The freshly cut proximal edge of the flap is thinned and shaped, then sutured to the recipient area in a layered fashion. The donor area can be undermined and advanced toward the postauricular sulcus or left to heal by second intention. If both the posterior ear and mastoid are deepithelialized, either closing the donor site or covering one surface with a skin graft will prevent scarring of the ear to the scalp.
Complications of the PIF are rare and can usually be avoided by proper flap design, meticulous hemostasis, and proper postoperative wound care. Postoperative bleeding can be prevented with careful intraoperative hemostasis or gently wrapping the pedicle with a hemostatic dressing, such as Surgicel. In order to prevent infection and chondritis, patients may be placed on a prophylactic course of antibiotics. Nonsteroidal anti-inflammatory medications may assist with minimizing pain and inflammation.
Temporoparietal fascial flap The temporoparietal fascial flap (TFF) is a thin, pedicled flap useful to reconstruct large auricular defects. Often used for traumatic ear avulsion, the TFF may be used in staged ear reconstruction for vascular coverage of cartilage and cartilage grafts.35 Over 85% of the flap’s blood supply is derived from the STA, with the remaining perfusion delivered by the PAA and occipital artery.36
Prior to designing the flap, a history of surgery, trauma, and radiation to scalp/temporozygomatic regions should be excluded.37 A Doppler may be used to trace the path of the STA, which is most easily identified 1 cm anterior to the tragus. This vessel runs cephalically and then branches into frontal and parietal branches at the uppermost aspect of the pinna (typically 3 cm above the zygomatic arch). The superficial temporal vein and auriculotemporal nerve follow a similar course.
An incision is made over the course of the artery through skin to the base of the subcutaneous fat. The incision must not extend more deeply, since the artery runs on the superficial surface of the superficial temporal fascia. The superior portion of this incision may be designed with a Y-shape to increase fascial exposure. Bald patients and those with shorter hairstyles may find these incisions difficult to camouflage. The flaps are then carefully elevated leaving the temporoparietal fascia intact.
When an adequate surface area of the temporoparietal fascia has been exposed, the path of the temporal branch of the facial nerve should be identified. Elevating the temporoparietal fascia will cause ipsilateral brow paralysis if it extends over the course of the nerve. Pitanguay’s line from the tragus to the lateral brow may serve as a surface landmark to avoid nerve injury. The frontal branch of the facial nerve may also be traced from the tragus to a point that is 3 cm superior and 2 cm lateral to the superior orbital rim37 The flap is elevated in the loose areolar plane above the deep temporalis fascia. The flap’s pedicle is eventually narrowed to less than 2 cm as it approaches the helical root so that it may be easily mobilized and transferred toward the ear. The flap is sutured over the exposed cartilage, and a skin graft is placed on its outer surface. The donor site is repaired in a layered fashion. Since the TFF is a pliable flap, the pedicle may not be conspicuous. However, a bulky pedicle may be detached 3 to 4 weeks after the initial inset.
CONCLUSIONS
Successful auricular reconstruction begins with preservation of patient hearing by ensuring EAC patency. Restoration of the oval ear silhouette and its relative position to the temporal scalp facilitates optimal cosmesis. Thorough knowledge of periauricular anatomy allows for localization of the facial nerve’s main trunk and also maximizes the use of adjacent tissue to reconstruct challenging defects.
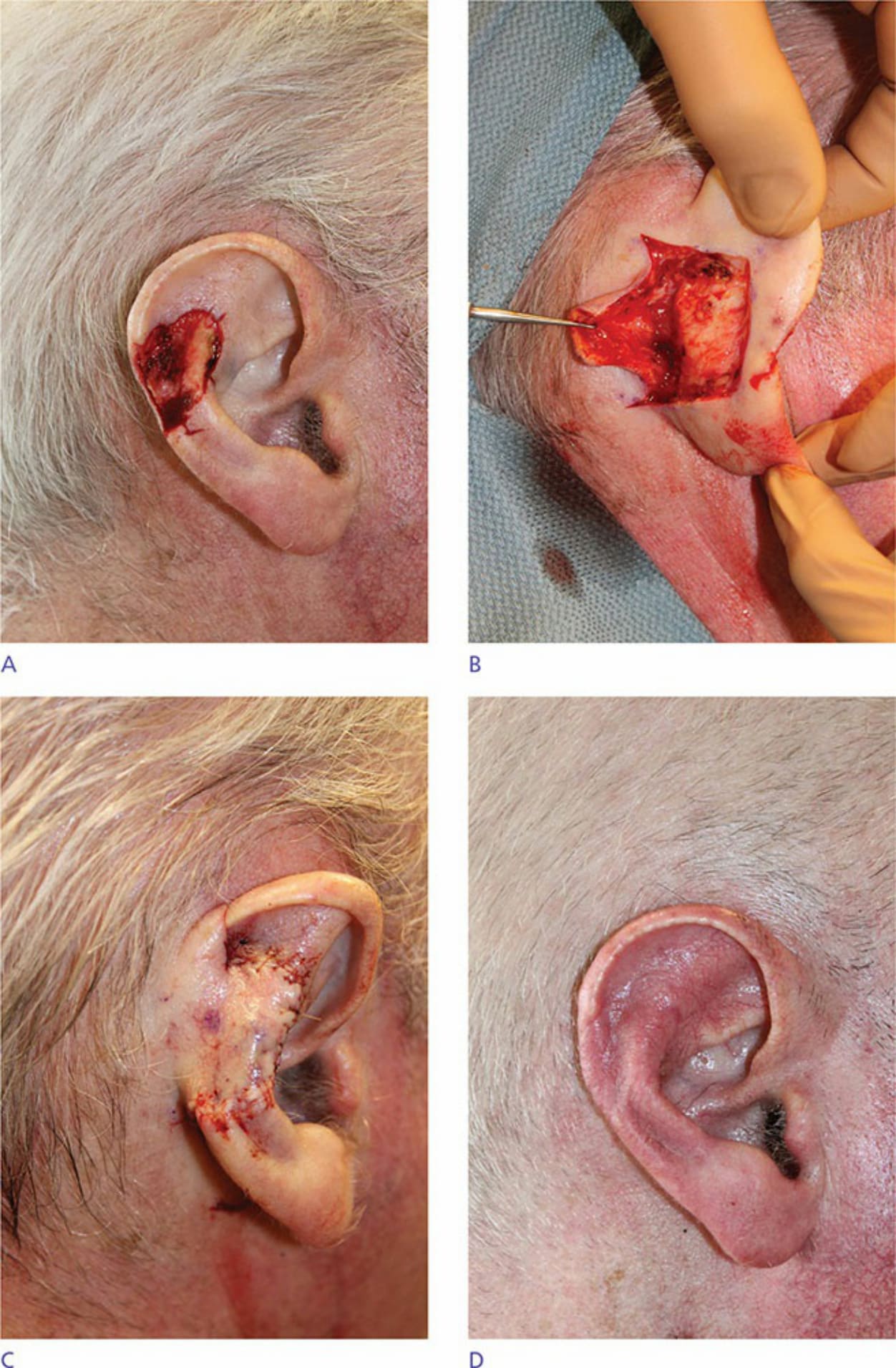
Figure 41-24. (A) Broad anterior auricular defect. (B) Postauricular interpolation flap incised and elevated above perichondrium. (C) Postauricular interpolation flap inset. (D) Two months postoperatively after postauricular interpolation flap separated.

Figure 41-25. (A) Full-thickness helical rim defect. (B) Cartilage graft inset for volume and stabilization. (C) Postauricular interpolation flap elevated above mastoid fascia. (D/E) Postauricular interpolation flap division. (F) Three months postoperatively after postauricular interpolation flap separated.