Transposition flaps
Transposition flaps
Transposition flaps are useful when tension at the primary defect precludes linear
closure or a sliding flap. They redirect tension away from the primary defect to adjacent tissue reservoirs. Since elevating and mobilizing the tight skin of the ear is usually not possible, transposition flaps of the ear must recruit skin from periauricular reservoirs. The skin of the mastoid scalp is relatively inelastic and contains a small zone of hairless postauricular skin; therefore, most transposition flaps of the ear recruit from the loose and mobile reservoir of preauricular skin. Regardless of the periauricular donor site, the transposition flap must cross either the deep postauricular sulcus or less prominent preauricular sulcus, which may result in tenting or contour deformity as the flap extends to the primary defect.
Banner flap The elongated rhombic flap, also known as a Banner flap, is a workhorse repair for helical root and upper helical rim defects. This random pattern flap transposes skin with a similar color and texture match from the pre- or postauricular skin to the ear (Fig. 41- 21). Perforator vessels from the STA or PAA supply these flaps.28 A flap similar to the Dufourmental rhombic flap is drawn from the defect along the pretragal or postauricular crease.29 The width of the flap and defect should match. As with other periauricular flaps, the Banner flap is elevated and undermined immediately above the SMAS. A larger length:width ratio risks ischemia, since the flap has a narrow pedicle. The key stitch, which bears the greatest tension, closes the donor site along the pre- or postauricular crease, and the flap is transposed with relatively low tension to the primary defect. Closing the donor site brings the beard or occipital hair closer to the pinna and may be a nuisance for patients to shave or trim.
Chondrocutaneous transposition flap Large full-thickness defects of the superior pinna can be repaired with a single-stage conchal bowl transposition flap (Fig. 41-22).30 A branch of the STA courses along the crus of the helix superficial to the cartilage31 and is included in the narrow, mobile, and robust flap pedicle. The anterior skin and cartilage are incised nearly 300 degrees from the cymba conchae along the antihelical rim to the inferior aspect of helical crus. The incision spares the EAC and preserves the entire helical crus, which forms the flap pedicle. The outer curve of the incision will become the new superior helical rim. The anterior skin and cartilage flap is elevated from the posterior auricular skin and rotated superiorly to replace the missing superior pinna. The flap lifts easily along the natural plane between the perichondrium and the skin of the posterior auricle. The conchal bowl donor-site defect is repaired with a skin graft. If the postauricular skin is intact, a postauricular island pedicle flap can also be considered to repair the conchal bowl donor-site defect. If there is additional exposed cartilage along the helical rim and scaphoid fossa, the remaining defect can be repaired with a postauricular interpolation flap (PIF) (Fig. 41-23).
Bilobed flaps Bilobed flaps have been described for postauricular and helical rim reconstruction.32,33 They can be conceptualized as transposition flaps with a significant rotational component, and as such may be useful when recruiting skin from the postauricular sulcus for helical rim defects.
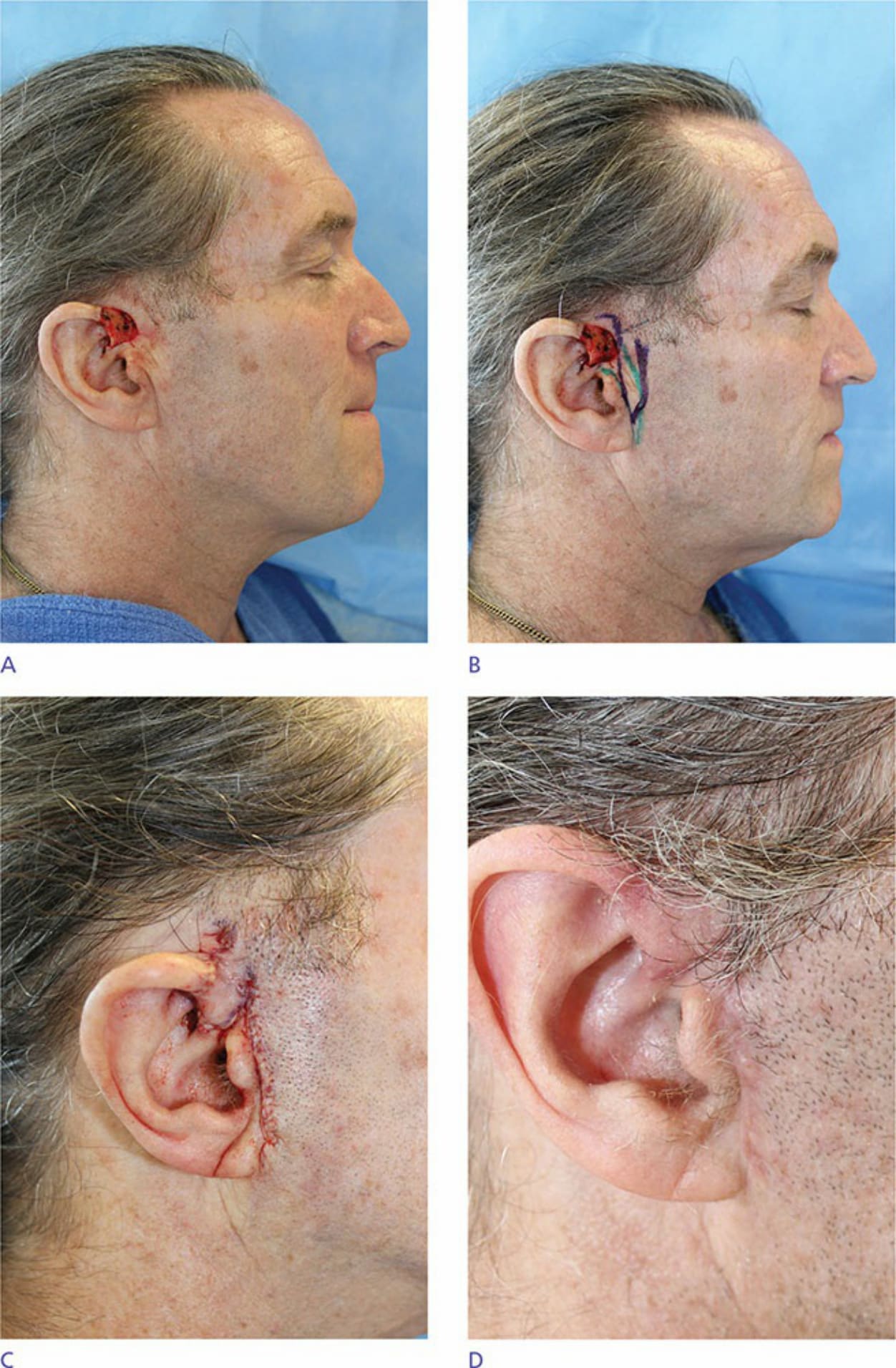
Figure 41-21. (A) Helical root defect. (B) Superiorly based Banner flap design. (C) Postoperative appearance. (D) Two months postoperatively.
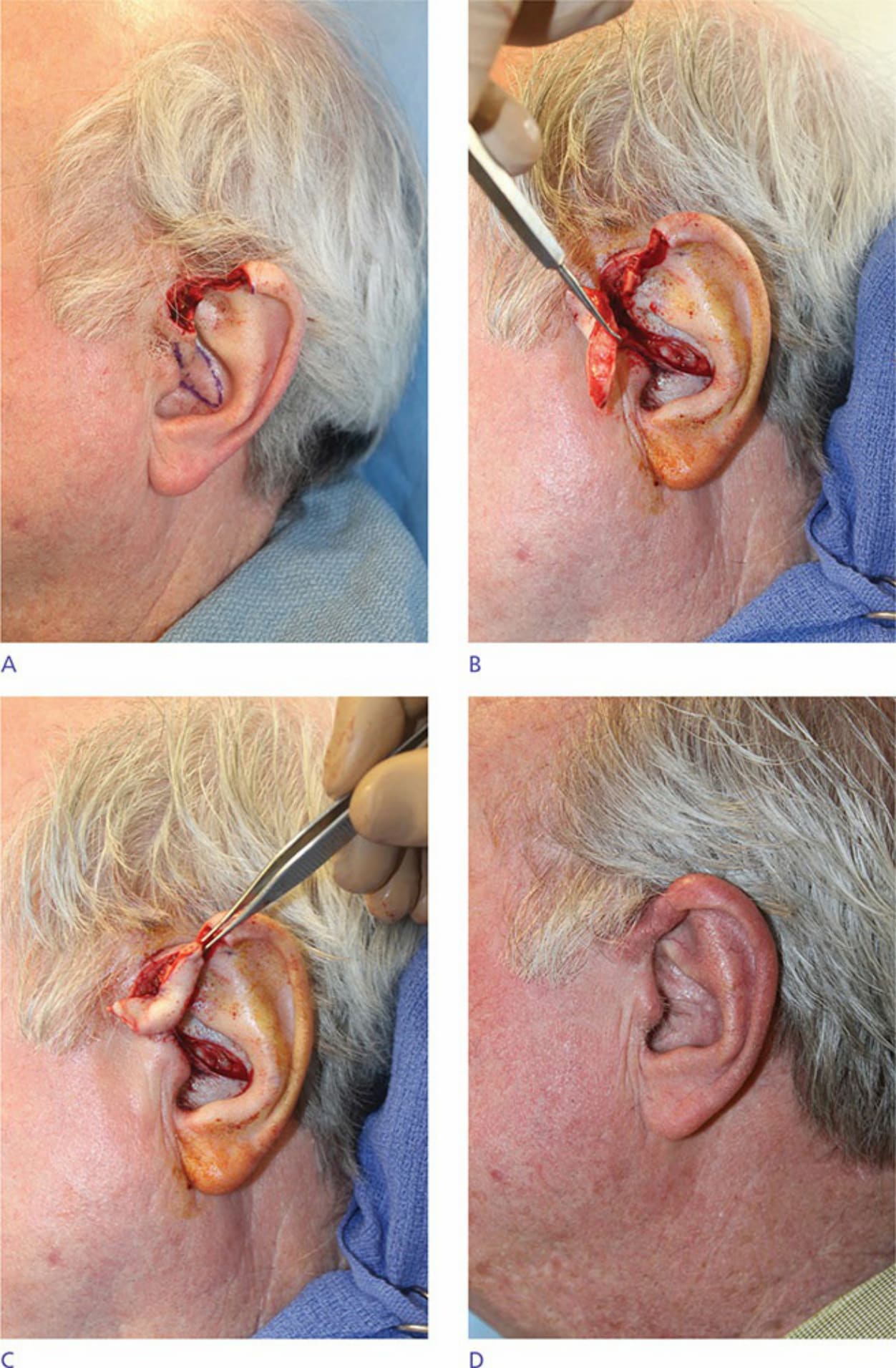
Figure 41-22. (A) Full-thickness helical rim defect with composite flap design based off helical root. (B) Skin and cartilage transposition flap elevated. (C) Composite flap transposed to reach upper helical rim with intact skin pedicle based at helical root. (D) Three months postoperatively.

Figure 41-23. (A) Full-thickness helical rim defect with exposed antihelical cartilage. (B) Skin and cartilage transposition flap elevated with pedicle based at helical root. (C) Skin and cartilage transposition flap transferred. (D) Postoperative appearance with postauricular flap covering antihelical defect. (E) Two months postoperatively after postauricular interpolation flap separated.