Flaps
Flaps
Because the thin skin of the anterior ear adheres to the cartilage, flaps may be used to mobilize the thicker, looser skin of the helical rim and posterior ear. Common examples on the ear include helical advancement flaps and V-Y island pedicle advancement flaps. Rotation flaps are infrequently performed on the ear.
Helical rim advancement flaps Helical rim advancement flaps are workhorse reconstructions for full-thickness, short helical rim defects (usually less than 1.5 cm). These flaps recruit skin from the loose, mobile earlobe. The earlobe-based advancement flap (ELBAF) incises a full-thickness tube of skin and cartilage along the scaphoid fossa from the lower margin of the defect
to the earlobe (Fig. 41-15E).15 The tube may be widened at the earlobe to enhance the blood supply. The narrow tube contains STA branches that course through the earlobe and run superiorly along the helical rim. A buried suture along the leading edge of the tubular flap advances the flap superiorly and closes the helical rim defect. The vertical arms of the flap are closed in a layered fashion. Advancing the flap may cause tissue redundancy along the inner edge of the vertical arms, and the standing cone can be excised at the earlobe. The ELBAF design may be modified with a bilateral tubular advancement flaps along the helical rim above and below the defect. This bilateral design offers limited mechanical advantage, because the inelastic skin of the superior limb has limited mobility and causes cartilage buckling.
Another modification of the traditional helical rim advancement flap is the chondrocutaneous advancement flap (Fig. 41-16).25 This flap also recruits skin from the loose earlobe, though the chondrocutaneous advancement flap has a broader pedicle derived from the posterior auricular skin. An incision is made from the inferior aspect of the helical rim defect along the scaphoid fossa to the earlobe through the anterior skin and cartilage. The postauricular skin is preserved and elevated immediately superficial to the cartilage on the posterior ear. A buried suture along the leading edge of the flap advances the flap superiorly and closes the helical rim defect. The vertical arm of the flap in the scaphoid fossa is closed in a layered fashion. Advancing the flap causes tissue redundancy along the inner edge of the scaphoid fossa, and a standing cone is excised at the earlobe. To avoid buckling when closing taller helical rim defects, removing a vertical strip of scaphoid cartilage may be necessary.26 Closing larger defects predictably shortens the height of the earlobe (Fig. 41-17).
V-Y Island pedicle advancement flaps Deep wounds located on the helical root (Fig. 41-18) and conchal bowl (Fig. 41-19) can be elegantly repaired with V-Y advancement flaps. Unlike other advancement flaps, the pedicle of V-Y flaps is perfused from a centrally located fasciocutaneous segment. This enhanced blood supply permits the flap to deliver thicker portions of tissue to the defect. The V-Y flap is designed by creating a triangular flap off of the defect toward the reservoir of skin to be lifted. Incisions are carried through the skin to the fascia, creating
an island. The flap is mobilized with circumferential undermining so the central 30% to 50% of the flap is tethered to the underlying tissue. The flap rocks forward toward the defect and should be sutured under minimal tension.
Pull-through flaps Deep defects of the concha and antitragus can be reconstructed with an island pedicle that pulls skin from the postauricular sulcus and mastoid areas into the defect (Fig. 41- 20).27 In order to mobilize tissue and minimize free margin distortion, the flap is measured exactly to the size of the defect. The medial aspect of the flap is positioned in the postauricular sulcus and provides both the blood supply and pivot point for the flap. After the flap is incised through the deep subcutaneous layer it is then undermined in this plane toward the sulcus, making certain to preserve soft tissue tethered to this pivot point. Next, a slit measuring the vertical height of the flap is created through the full thickness of skin (and cartilage if still intact) just lateral to the EAC. After meticulous hemostasis is obtained, the lateral edge of the mastoid skin is elevated, pulled through the full-thickness opening, and laid atop the defect. Cartilaginous grafts may be used under the flap to support the auricular framework if the defect extends closer to the helical rim. The secondary defect is sutured to recreate the postauricular sulcus and the flap may be secured to the defect with sutures. Patients may report a sensation of the ear being pulled back if the flap is used to cover a wide horizontal distance.
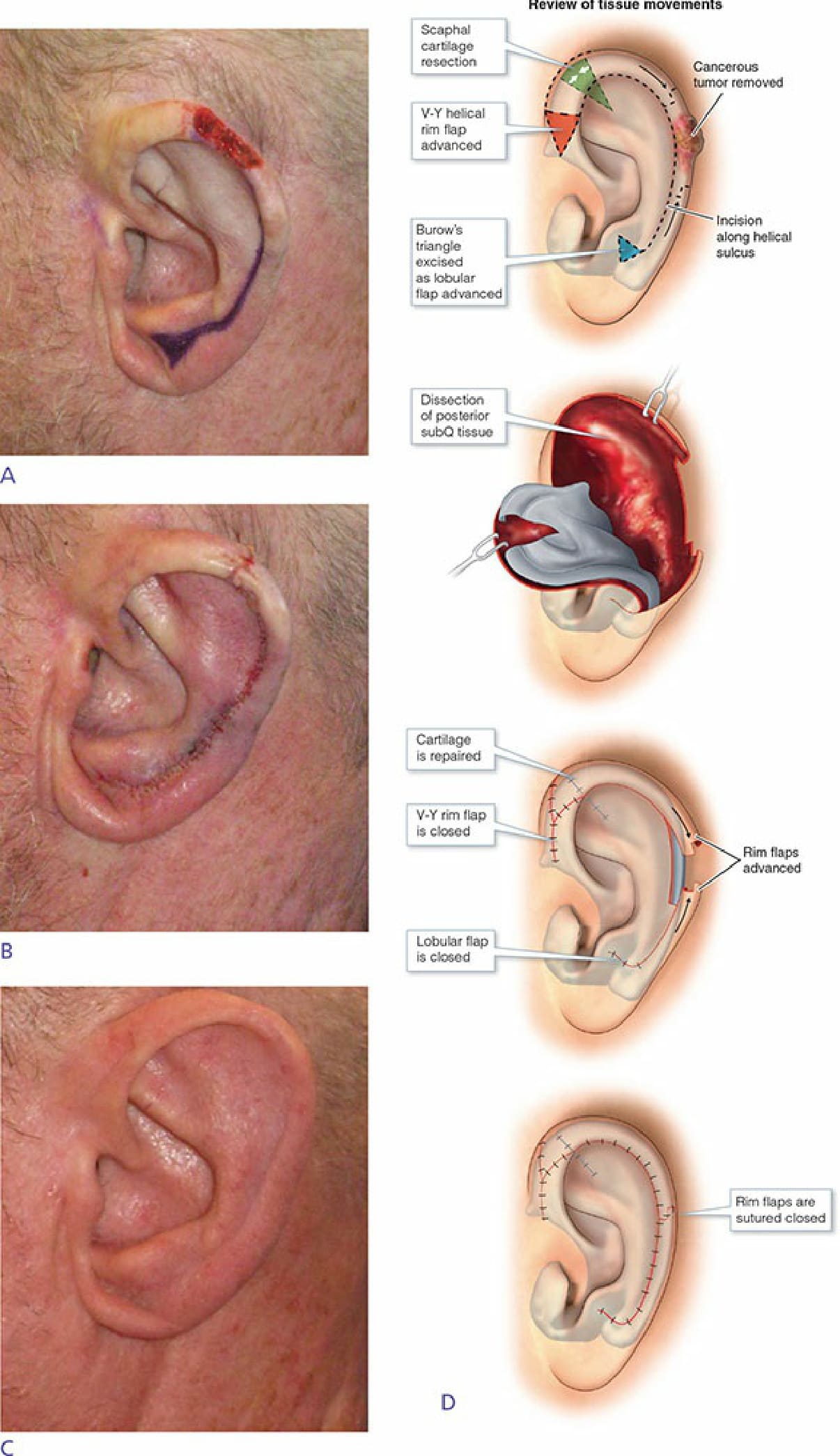
Figure 41-16. (A) Helical rim defect. (B) Chondrocutaneous advancement flap design that hides incision within scaphoid fossa. (C) Postoperative appearance. (D) Figure illustrating the chondrocutaneous advancement flap.

Figure 41-17. (A) Helical rim defect. (B) Chondrocutaneous advancement flap elevated off of cartilage framework. (C) Postoperative appearance. (D/E) Six-week postoperative appearance with frontal view revealing reduced earlobe height.
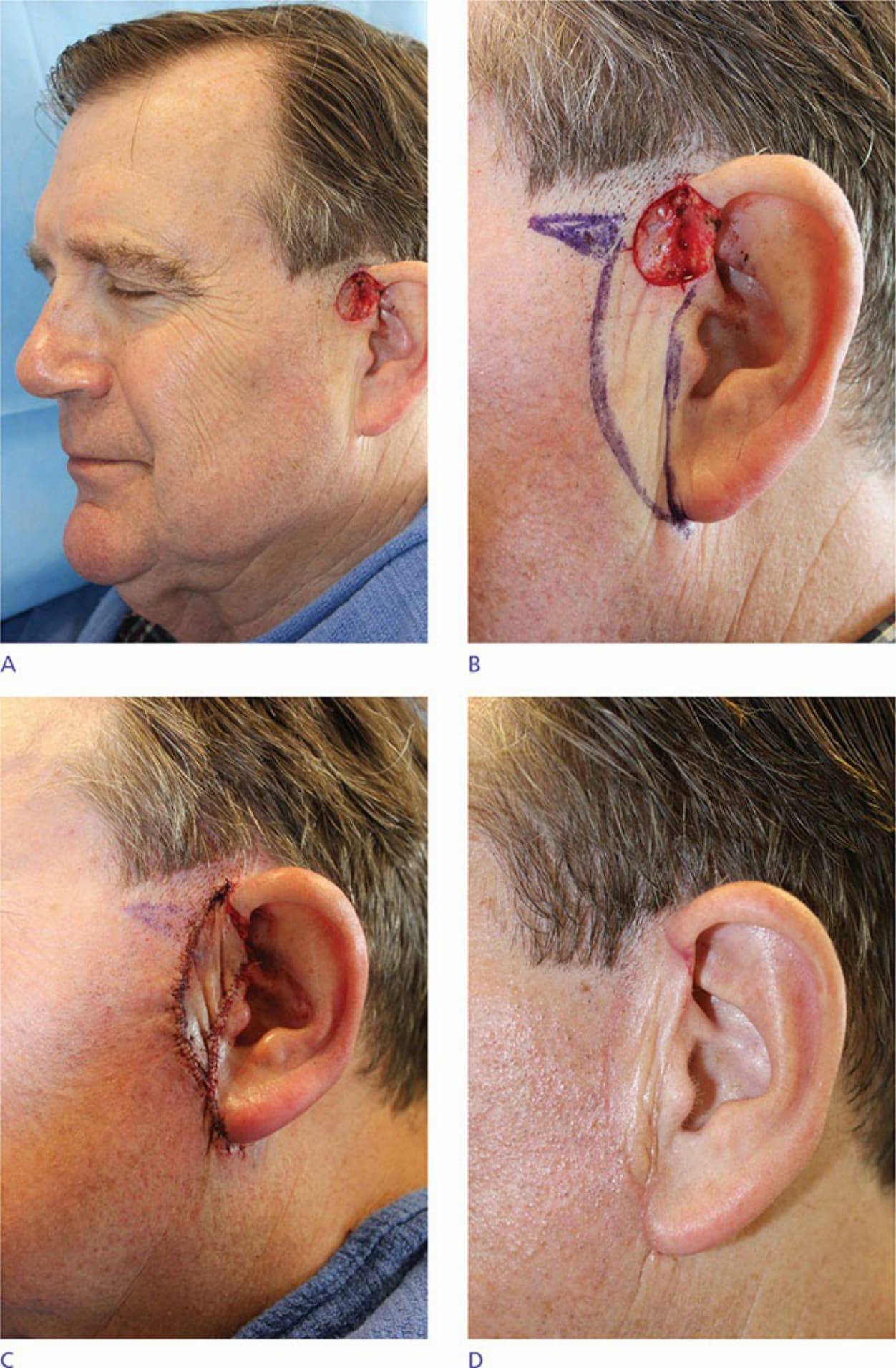
Figure 41-18. (A) Preauricular cheek defect. (B) Inferiorly based V-Y advancement flap design. (C) Postoperative appearance. (D) Three months postoperatively.
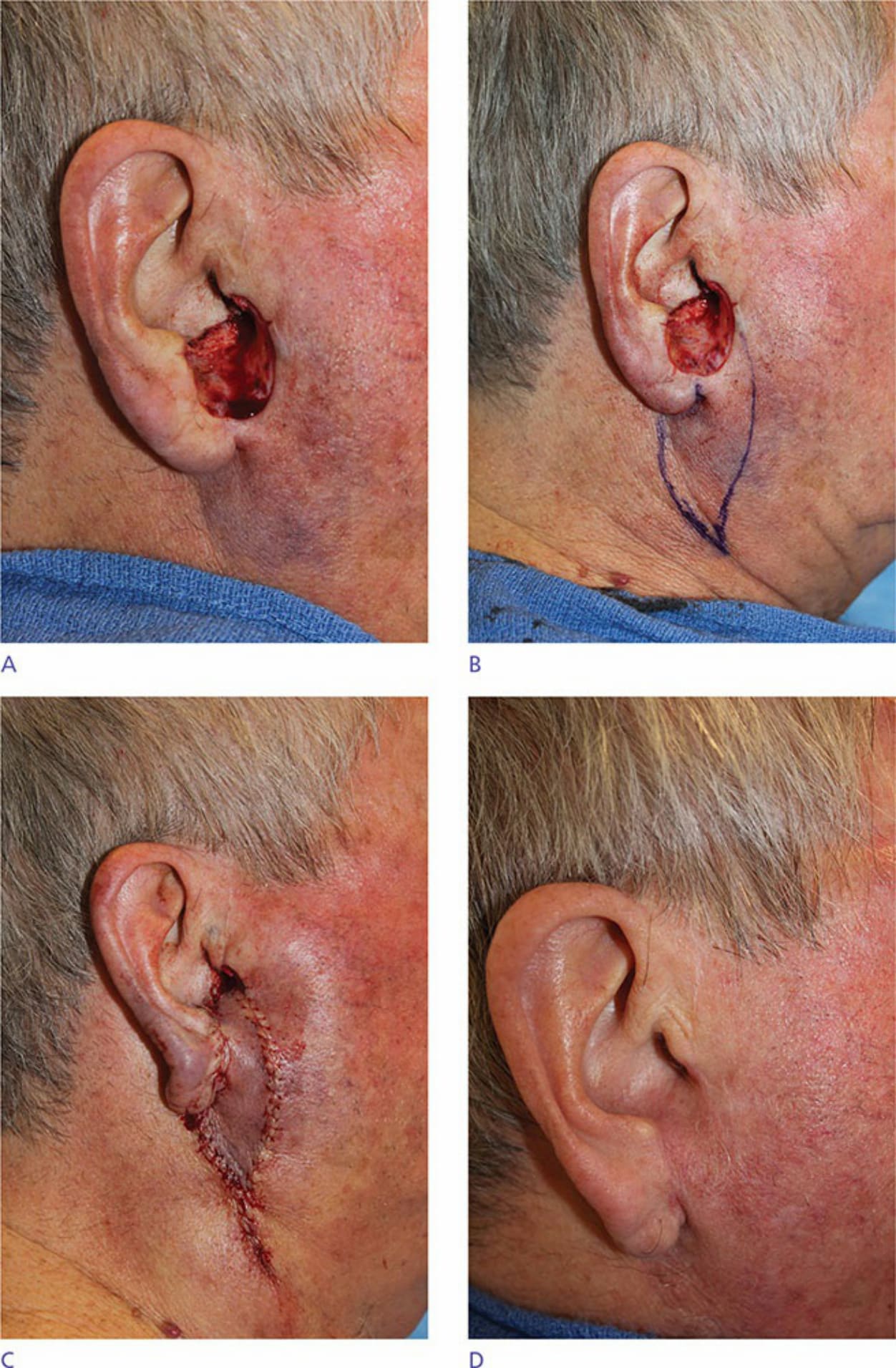
Figure 41-19. (A) Preauricular cheek and conchal bowl composite defect. (B) Inferiorly based V-Y advancement flap design. (C) Postoperative appearance. (D) Two months postoperatively.
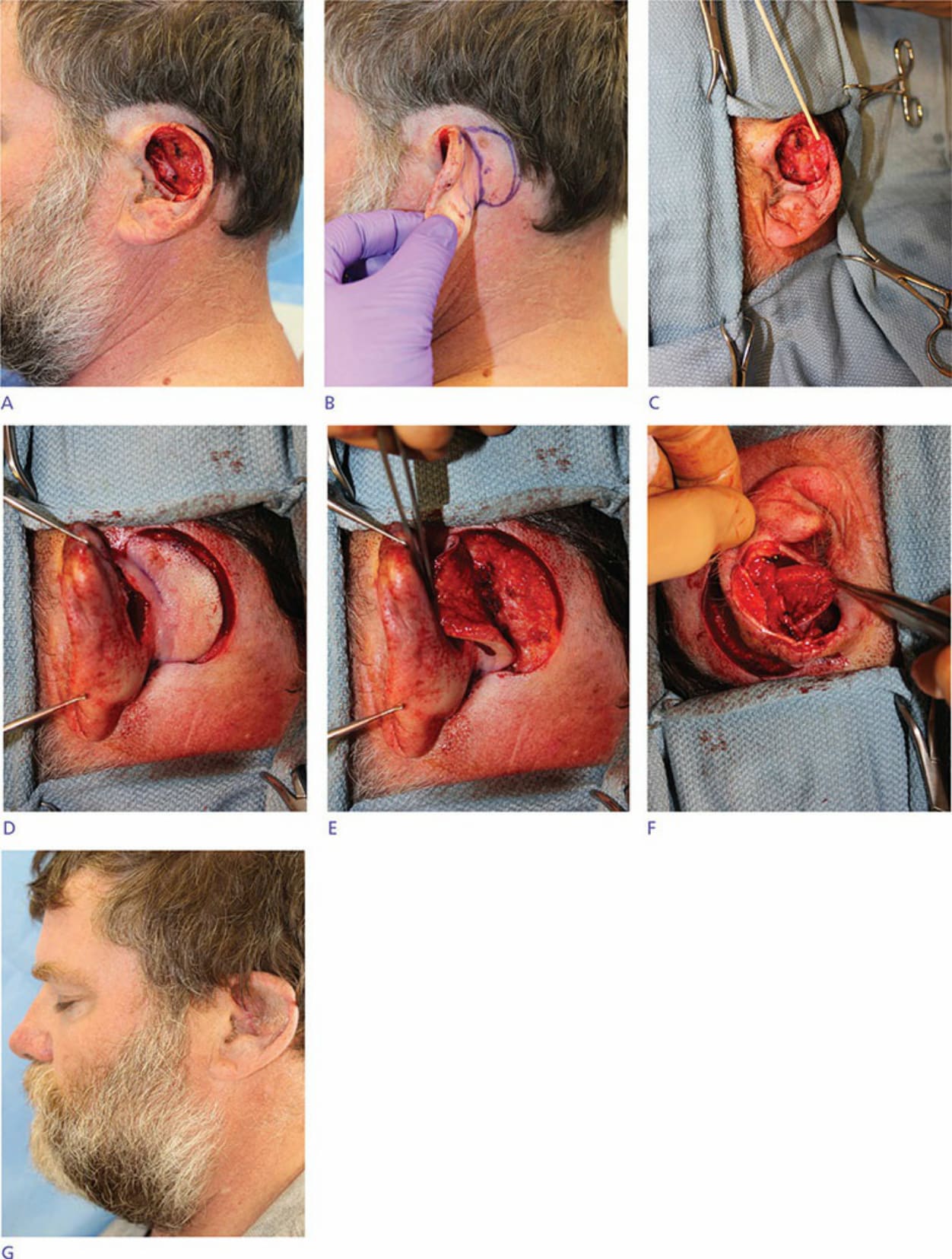
Figure 41-20. (A) Anterior auricular defect with absence of cartilage. (B) Pull-through V-Y flap design on postauricular sulcus. (C). Cartilage graft secured to anterior surface of ear for stabilization. (D) Pull-through V-Y flap incised. (E). Pull-through V-Y flap elevated. (F) Pull-through V-Y flap as it passes through full-thickness portal. (G) Two months postoperatively, note hairs from temporo-occipital scalp have been transferred to the ear.