Wedge repairs
Wedge repairs
Wedge repairs are useful to restore contour of full-thickness helical rim defects, ideally less than 1 to 1.5 cm in height. Wedge repair of taller rim defects may noticeably decrease the height of the ear. The wedge repair is analogous to one-half of a linear closure. Two arms of a triangular standing cone are drawn from the edges of the rim defect toward the center of the ear, where they converge at an angle of 30 degrees or less. The full thickness of the triangle, or “wedge,” is excised. On the pinna, the wedge includes the cartilage and skin (Fig. 41-13). On the earlobe, the wedge includes the skin and subcutaneous fat (Fig. 41-14). The first suture, or key suture, realigns the free edges of the wedge along the helical rim with everted edges to avoid notching. Buried sutures with the knots on the postauricular side reapproximate the cut edges of cartilage. Wide bites that grasp the dermis on one or both sides may be necessary to avoid tearing the cartilage. Anteversion or forward cupping of the ear may occur and can be minimized by resecting star-shaped composite segments (Fig. 41-15), rather than the simple triangular wedge. After realigning the cartilage edges, the skin can be closed with a simple layer of running sutures.
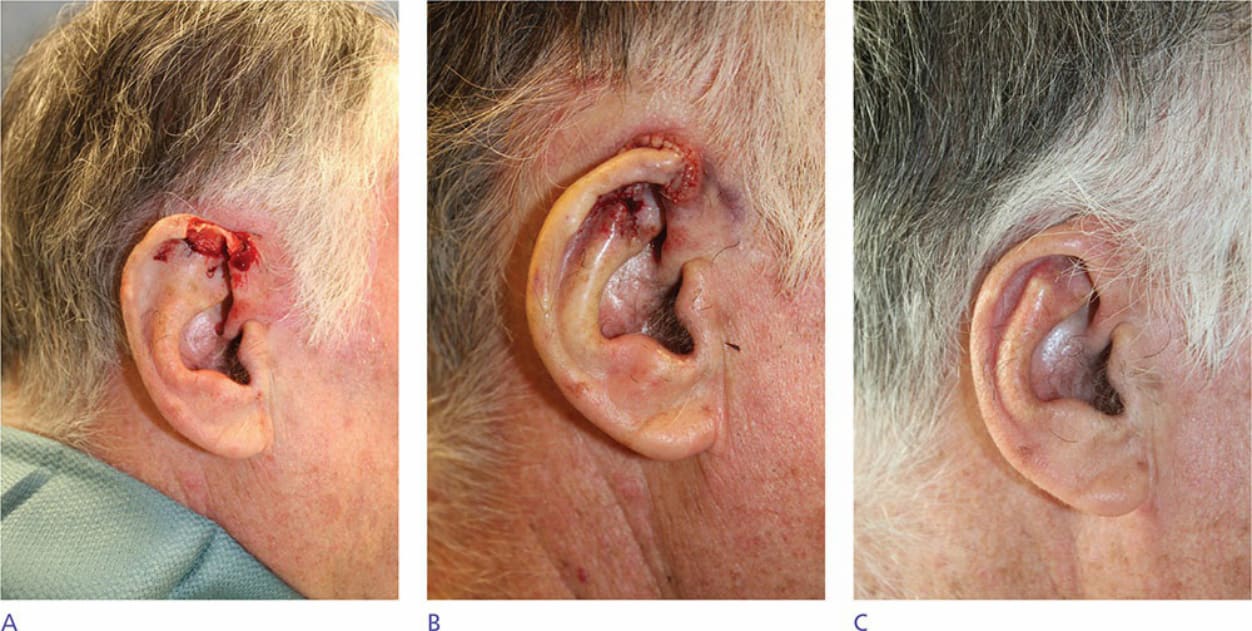
Figure 41-13. (A) Helical rim defect. (B) Wedge repair. (C) Two months postoperatively.
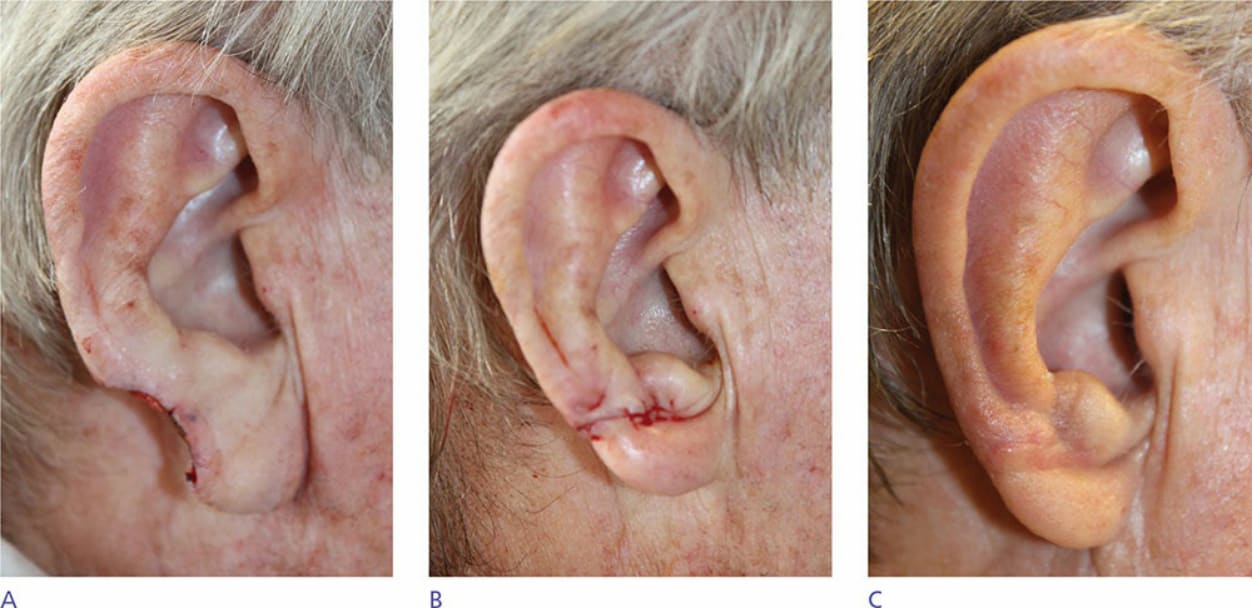
Figure 41-14. (A) Earlobe defect. (B) Wedge repair. (C) Two months postoperatively.
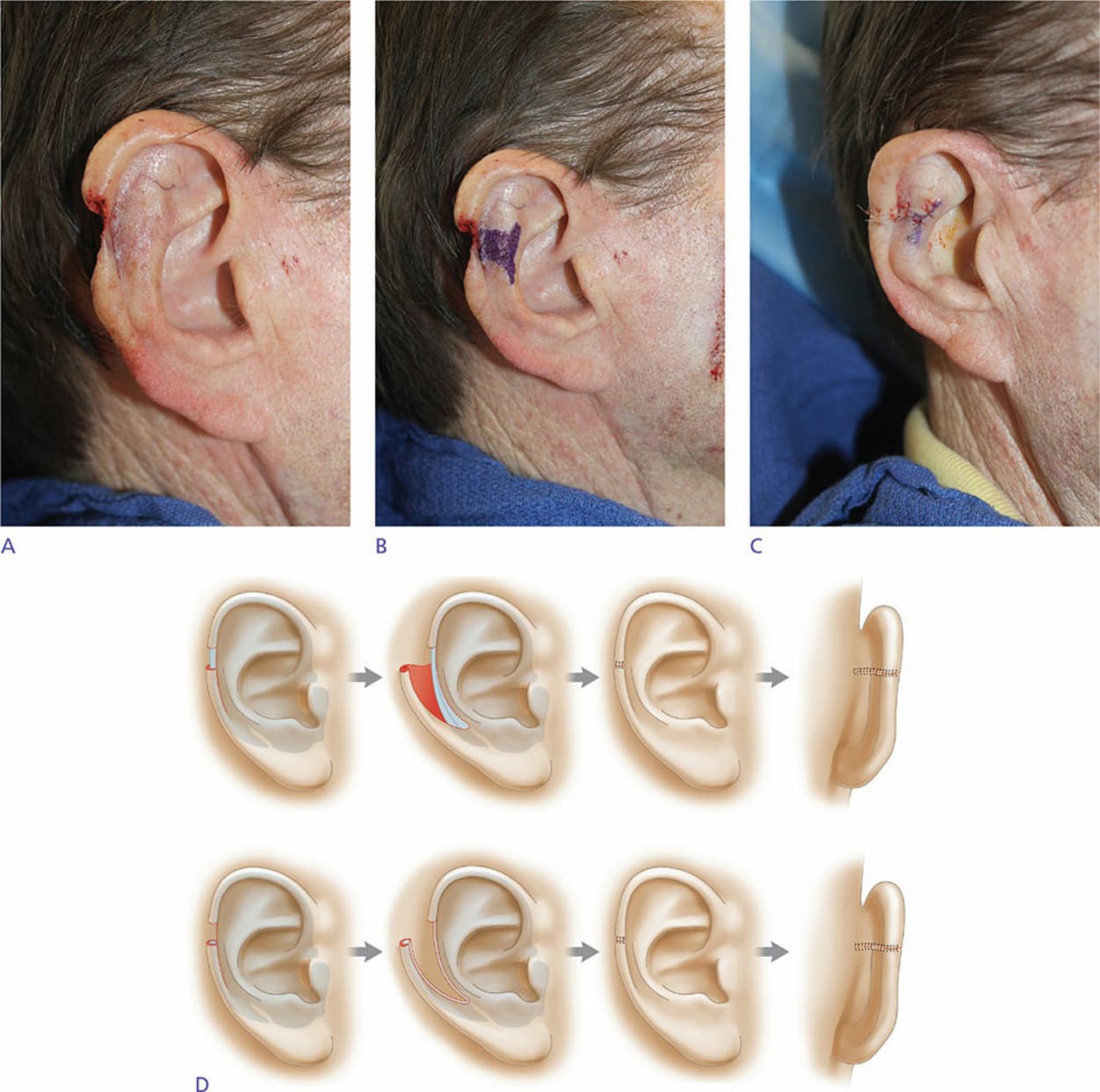
Figure 41-15. (A) Helical rim defect. (B) Star-shaped wedge design. (C) Wedge repair. (D) Illustration of the helical rim advancement flap.