Skin grafting
Skin grafting
Skin grafting plays a large and versatile role in auricular reconstruction. Nearly any partial-thickness ear defect with preserved perichondrium is amenable to skin grafting (Figs. 41-7 to 41-9). Full-thickness skin grafts (FTSGs) have increased metabolic demand but provide greater volume, which may be desirable to restore contour of helical rim defects.23 The pre- and postauricular skin folds are ideal donor sites for small FTSGs because of similar sun exposure, sebaceous gland density, and dermal thickness (Fig. 41-10). Postauricular donor sites may decrease operating time, since they do not require primary closure. Split-thickness skin grafting may be preferable if the blood supply at the base of broad wounds is tenuous (Fig. 41-11).24
Grafts placed on wounds with insufficient blood supply or that do not conform to the complex topography of the ear have an increased risk of necrosis. Cartilage stripped of perichondrium will not adequately nourish a skin graft. One strategy to provide a vascularized wound bed is to cut a window of the stripped cartilage so that the graft can be sutured to the highly vascularized skin on the other side of the ear (Fig. 41-11A). Excising the cartilage of the concha and antihelix will rarely change the shape of the ear if at least 1 to 1.5 cm of the outer helical rim is intact. Air pockets between the graft and wound base will cause necrosis or infection. Quilting sutures and/or conforming bolster dressings eliminate this dead space and conform skin grafts to the concavities and convexities of the ear (Fig. 41-12).

Figure 41-7. (A) EAC defect. (B) Immediate postoperative appearance.

Figure 41-8. (A) Conchal defect. (B) Two months postoperatively.

Figure 41-9. (A) Antihelical defect. (B) FTSG in place with quilting sutures to recreate the scaphoid fossa. (C) Two months postoperatively.
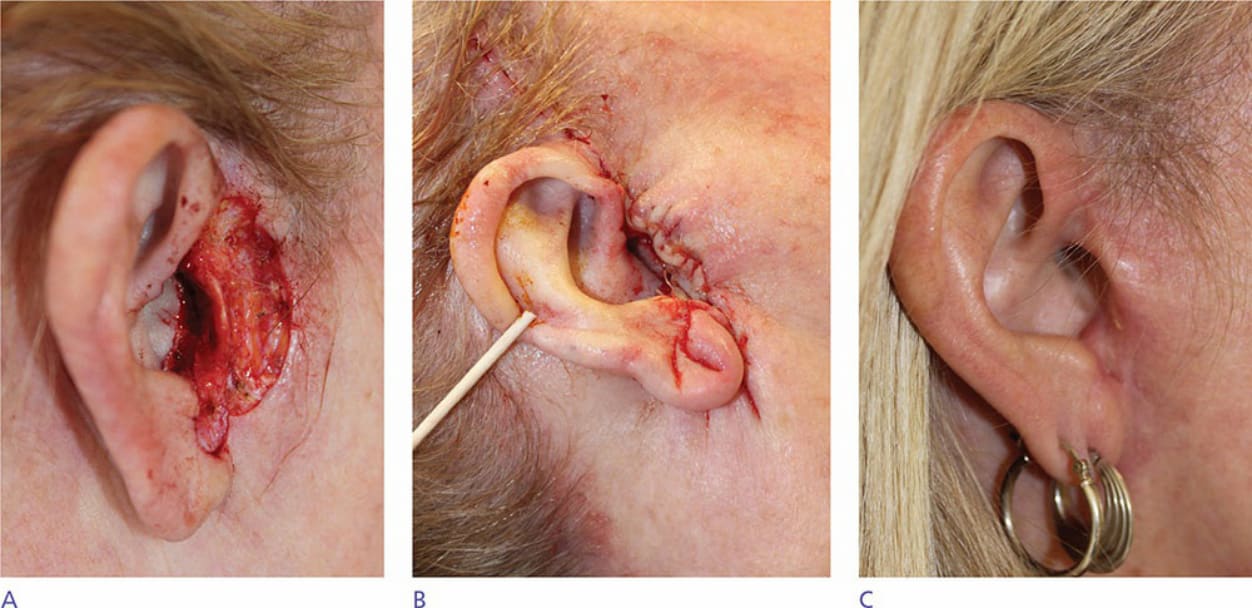
Figure 41-10. (A) Pretragal and EAC defect. (B) Preauricular skin advanced and redundant cones used for EAC graft. (C) Four months postoperatively.
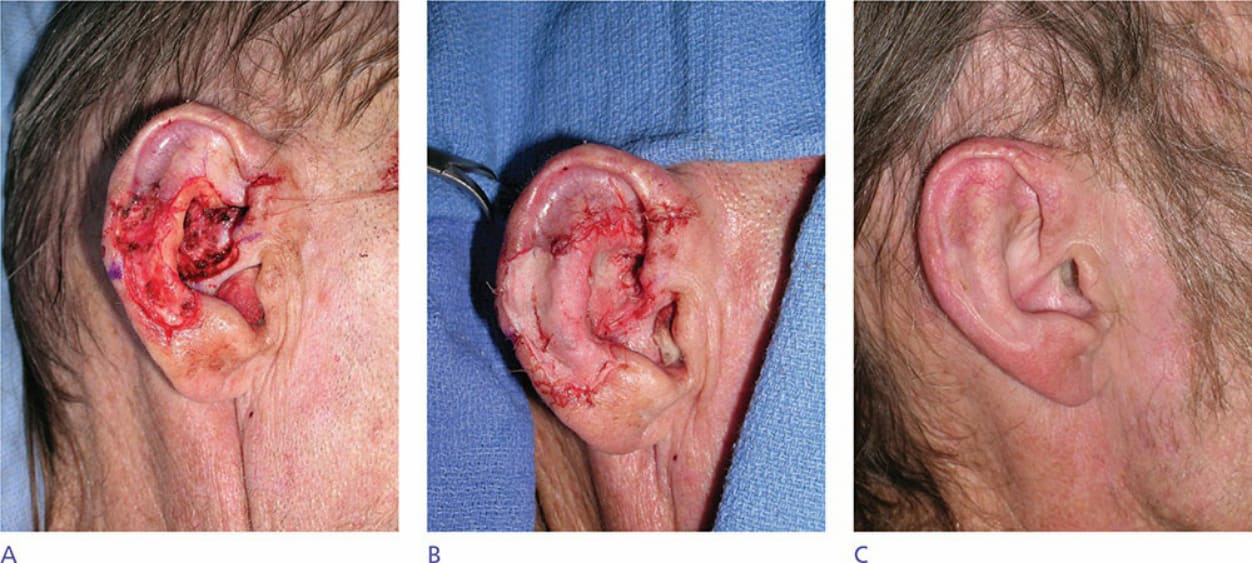
Figure 41-11. (A) Defect spanning antihelix and concha. Note that a window of cymba conchae cartilage devoid of perichondrium was excised to facilitate graft survival. (B) Split-thickness skin graft sutured to wound. (C) Eight months postoperative appearance with expected hypopigmentation of graft.

Figure 41-12. (A) Numerous quilting sutures placed in center of full-thickness skin graft to minimize dead space from wound bed. (B) Xeroform bolster fixed to wound with through-through suture further ensuring contact between graft and wound bed.