Nasolabial flaps
Nasolabial flaps
Inferiorly based nasolabial flaps can be used to resurface very large operative wounds of the lateral upper lip subunit.9,15 Appropriate defects are those that are very long in a horizontal plane and which do not involve the lip margin. The flap is designed along the nasofacial sulcus superiorly toward the medial canthus. As the cheek is closed, the flap transposes into place to repair the lip wound (Fig. 40-38). The reliable vasculature and easy mobility of this repair allow for predictable flap survival. This repair has the potential for two problems. It ablates the nasolabial fold, and the flap tends to be bulky and prone to pincushion. The bulkiness and pincushioning can be minimized by appropriate undermining of the recipient lip and by dramatic thinning of the flap prior to inset. The pedicle for a nasolabial flap is richly vascular; it can be reliably thinned to very superficial adipose. The nasolabial fold can be recreated at 6 months with a standard Z-plasty (Fig. 40-39).
Occasionally, a nasolabial interpolated pedicle flap can be utilized for large wounds of the upper lip without involvement of the nasolabial fold (Fig. 40-40). The flap is elevated, much as in the single-staged procedure, but then bridged over the recreated
nasolabial crease. A thin and mobile pedicle is usually well vascularized. The flap can then be thinned dramatically at the time of take down in 2 to 3 weeks. A period of pincushioning is to be expected, and revision may be needed.

Figure 40-38. Nasolabial transposition flap to repair an upper lip wound. (A) An oval horizontal wound presents a reconstructive challenge. (B) An inferiorly based nasolabial flap is designed. (C) The flap has been elevated and sutured into place. This will ablate the nasolabial fold upon healing.
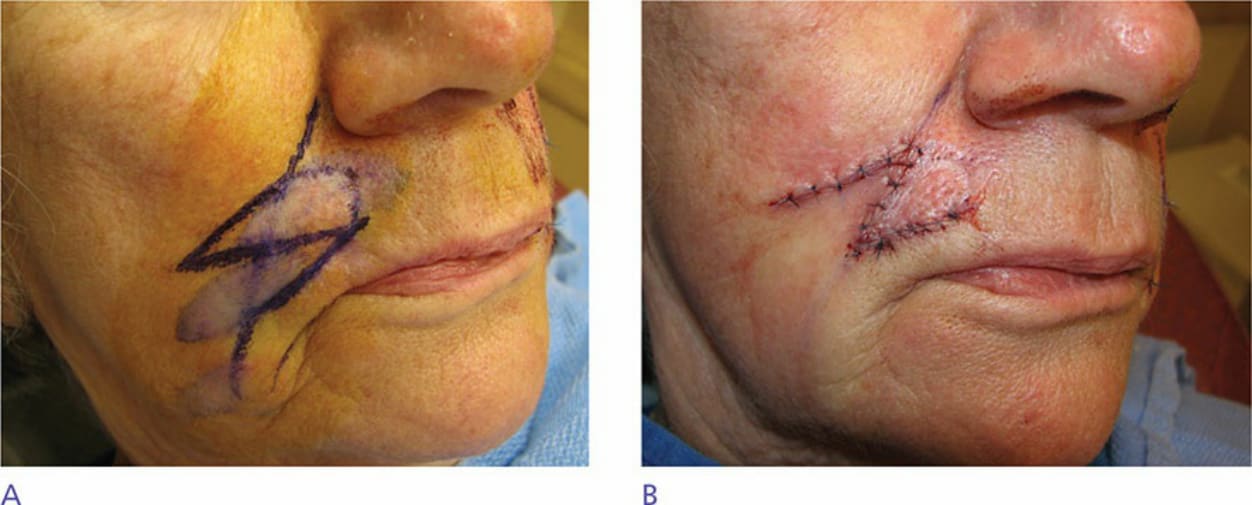
Figure 40-39. Revision to recreate a nasolabial fold. (A) A flap has ablated the nasolabial fold. A Z-plasty is designed to recreate the fold. (B) The Z-plasty is transposed and sutured into place.

Figure 40-40. Extensive upper lip wound repaired with a partial lip wedge, a mucosal island flap, and a cheek to lip interpolated pedicle flap. (A) Very large upper lip wound demands a creative approach. (B) About one-third of the repair is designed and implemented as a full-thickness lip wedge. (C) The wedge is closed, making the wound manageable, and an inferiorly based nasolabial interpolation flap is designed. The mucosal lip has been advanced. (D) The nasolabial flap has been elevated, and the cheek wound repaired.