Island pedicle flaps
Island pedicle flaps
Island pedicle flaps are excellent repairs for defects of the lateral upper lip and apical triangle (Fig. 40-35).11–13 Even substantial operative wounds can be reliably closed with an island flap based on the perforators of the orbicularis oris and surrounding perioral vascular plexus. Island pedicle flaps are most valuable when one or more limbs of the flap can be hidden along a pre-existing line. If all three lines of the flap are visible “floating” on the lateral upper lip, the result is not aesthetic. Modest wounds of the apical triangle are particularly well suited to the island pedicle flap, as the outer limb of the flap is hidden within the nasolabial fold. In some cases it is useful to enlarge the operative wound to encompass the entire apical triangle region. Such repairs should be designed with adequate width to allow for closure of the operative wound without tension along a secondary vector. The length of the flap is tailored to allow for the advancement needed for the primary motion to close the operative wound. In general a longer flap is easier to elevate, advance, and suture. A Z-plasty modification of the lower horizontal line can enhance results (Fig. 40-14A–C).14
Labial island pedicle flaps are incised just to the underlying orbicularis oris. The surrounding tissues should be undermined just above muscle. The advancing margin of the flap must be undermined to avoid a “bulldozing” phenomenon and the posterior, lateral, and inferior restraints must be meticulously freed. In order to achieve an aesthetic repair the flap should advance under little tension. A small but well-mobilized pedicle is favored over a bulky, adherent one. Slightly insetting the island and undermining the remaining lip widely can minimize pincushioning. Even when performed elegantly, some trap-door effect is common for these repairs, though this will reproducibly diminish with time. When the operative wound includes an undermined region of the nose, the advancing margin of the pedicle may be de-epithelialized and advanced under the remnant ala (Fig. 40-36).
Large, even extensive operative wounds of the upper lip can be repaired with an
island pedicle flap that straddles the nasolabial fold and extends out onto the cheek, lateral and inferior to the oral commissure (Fig. 40-37). This type of island flap is based not on the orbicularis oris, but on the richly vascularized adipose tissue of the medial cheek. Wounds of up to 3 cm can be closed readily with broad, large island flaps. In such cases, the flap is undermined entirely off the orbicularis oris. The lateral pedicle is preserved, and the trailing tension vector is completely severed. The skin of the cheek is dissected free of the pedicle at a shallower plane. This is a robust flap, as it pulls the facial artery medially with it as the wound is repaired. As noted above, peripheral undermining and a slight inset of the flap at suturing can diminish pincushioning in the postoperative period.
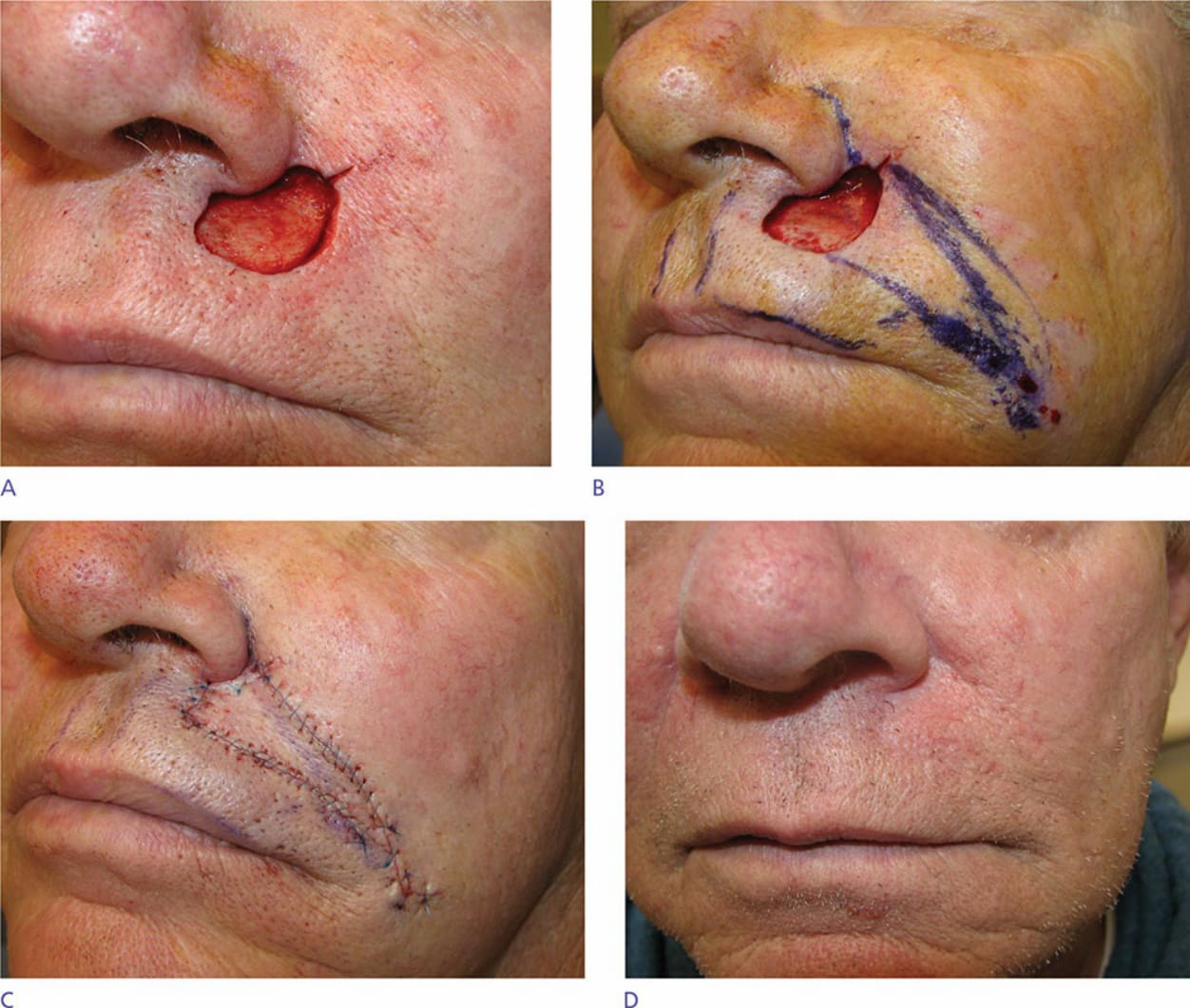
Figure 40-35. Classical repair of an upper lip wound with an island pedicle flap. (A) Wound of the left upper lip near the apical triangle. (B) Island flap design. The upper outer limb of the flap approximates the nasolabial fold. (C). The repair is advanced into place. The pedicle for this flap may be a deep muscular pedicle or a superolateral fatty pedicle. (D) Final result at 6 months.
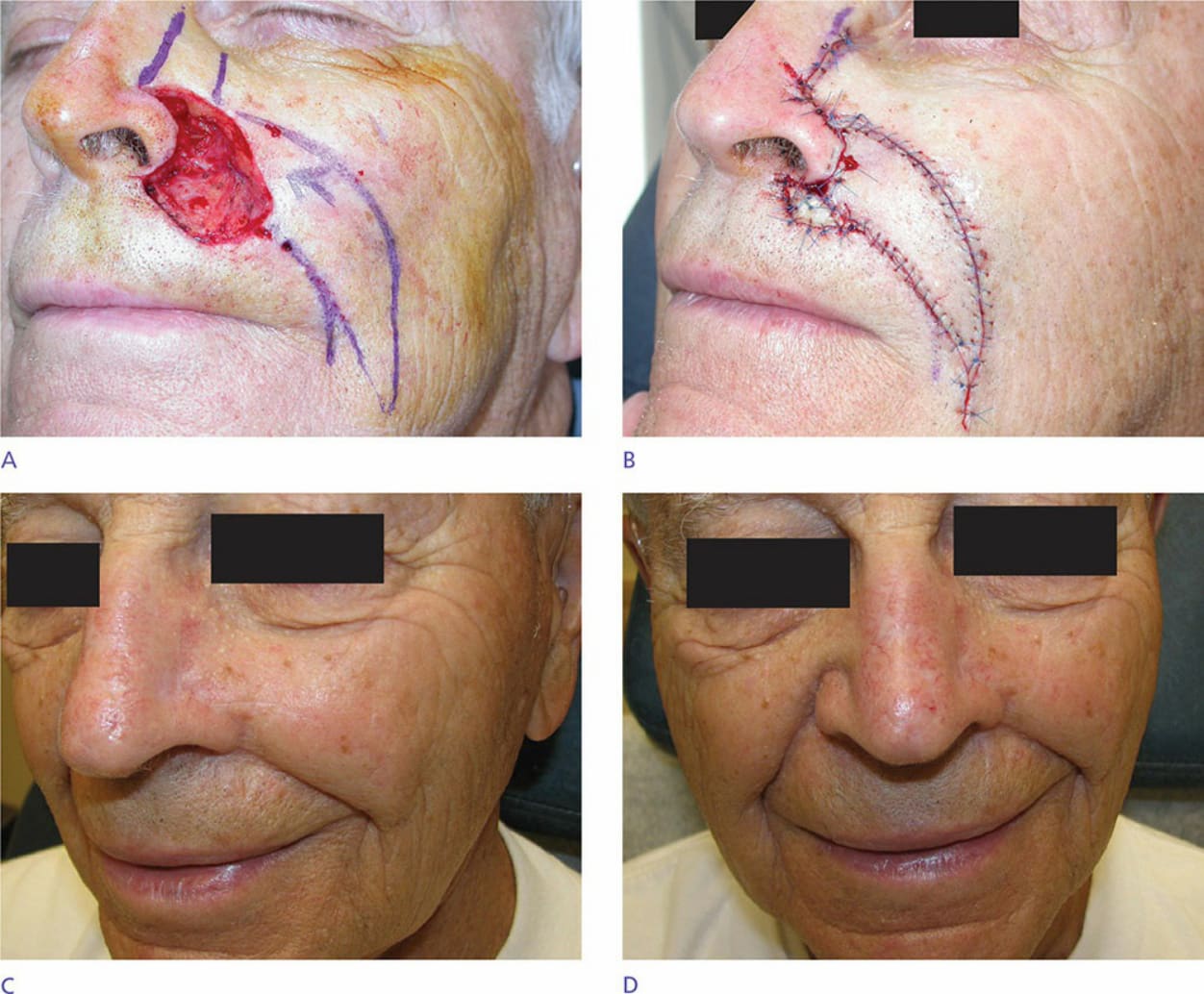
Figure 40-36. An island flap may be used to recreate a base for an undermined alar defect. (A) A large defect involves the apical triangle, much of the upper lip lateral subunit, and a small portion of cheek. A cheek advancement will close the defect of the nasofacial sulcus and an island flap is designed to repair the lip wound and stabilize the ala. (B) The cheek has been advanced medially and the island has been advanced underneath the ala to support it. The leading edge of the island has been de- epithelialized. (C) Repair at 1 year. (D) There is some asymmetry, as the apical triangle has been ablated and the nasolabial fold has been moved medially. This could be repaired with a Z-plasty if the patient so desired.

Figure 40-37. Very large wounds of the upper lip may be repaired with island flaps. (A) Large wound of the lateral upper lip. (B) Repair with a large cheek island flap based on a fatty pedicle.