Linear repairs
Linear repairs
Small and modest wounds of the mid-upper lateral subunit may be repaired linearly (Fig. 40-26). Vertical lines on the lip are common with age. With proper execution, such repairs can be highly aesthetic and lead to minimal or no functional impairment. The most appropriate wounds for a linear repair are those which lie above the vermillion border and whose vertical axis is longer than the horizontal axis. Linear repairs on the lip do not need to be exactly vertical. They generally should parallel the philtral columns medially but remain perpendicular to the vermillion border as it arcs slightly with its lateral procession. Linear repairs on the lip must be long and should be carried right through the vermillion border.3 In most cases, the outermost orbicularis band should be transected and excised as a “mini wedge,” without which a standing pucker of lip will often exist (Figs. 40-27 and 40-28). Dog ears on the lip do not recede, and therefore the repair must be long enough and deep enough (just above orbicularis) to ensure that it lies flat at the moment of closure. In addition, the sharper the defining line between the vermillion and cutaneous lip, the more meticulous must be the alignment of apposing wound margins. In patients with a well-defined white line, even mismatch of a millimeter or less of vertical height will create a visible deformity and ruin what may otherwise be a nearly invisible repair. Patients with a vaguely demarcated vermillion border “zone” require less meticulous vermillion border alignment.
Lip wedge Wounds involving the vermillion border of the lateral upper lip are common. Many such defects can be repaired with a full-thickness or modified full-thickness wedge reconstruction (Fig. 40-29).4 As originally defined, the wedge is a full-thickness Vshaped transmural repair. The operative wound edges are squared off and a fullthickness V-shaped “pie” of tissue is excised up to the gingival sulcus. The labial artery is either ligated or electrocoagulated, and the repair is then closed in a multilayer fashion. The mucosa is first closed with an absorbable suture such as plain gut. The muscle is then reapproximated with an absorbable buried suture, the dermis is separately repaired and then the epidermis and vermillion mucosa are reapproximated.
As with the simple partial-thickness closures, in patients with a sharply defined white line it is imperative to carefully match the vermillion borders. If the defect is broad and the lip narrow, a wedge will lead to a mismatch between the smaller lateral cutaneous lip and vermillion and the taller more substantive medial remnant. The result will be a functional lip but a visible mismatch. This may be a tolerable deformity but should be considered if the patient has high cosmetic expectations. A sliding Z-plasty
technique can effectively overcome this mismatch.5
A wedge reconstruction of any defect that encompasses more than one-quarter of the upper lip has the potential to cause microstomia; for larger wounds, combination repairs, rotational flaps, and lip-sharing procedures may be preferred. The advantage of a lip wedge is that it is a relatively nonmorbid repair with a low risk of complications. As with partial-thickness repairs, wedges need not be entirely vertical but should align with radial relaxed skin tension lines (RSTLs) that are typically perpendicular to the vermillion border.
Any vertical line scar on the upper or lower lip can demonstrate exaggerated creasing with time, due to repeated contraction of the orbicularis oris muscle. A Zplasty (traditional or sliding) incorporated into the vertical incision line of a linear repair, wedge, or flap acts as a strut that resists this creasing. When the Z-plasty is executed, the depth of incision for the arms of the Z-plasty is typically down to muscularis. In practice, the final horizontal central limb of the Z-plasty is not noticeable.5
A modification of the lip wedge avoids extending the repair all the way to the gingival sulcus and preserves some muscle (Fig. 40-30).6 In the modified technique, the external repair is extended the full vertical height of the lip, but the internal extent is only about 50% of the height of the lip. The distal band of orbicularis is completely severed, as is the labial artery, but the larger, deeper major circumoral band of orbicularis is preserved. This repair is less extensive than the full-thickness wedge and may preserve a more normal circumoral muscle tone in the postoperative period. From an aesthetic standpoint there seems to be little difference from the standard lip wedge.
Advancement Many moderate to large cutaneous wounds of the upper lip lateral subunit can be
suitably repaired with unilateral advancement flaps (Figs. 40-31 to 40-33).3,7–9 These large repairs use laxity from the medial cheek to allow for a nearly tension-free closure, thus avoiding philtral and vermillion distortion.
is an area with rich vasculature, and precise hemostasis is essential. (D) Immediate closure. The most challenging aspect of this repair is judging the effect of the advancement on the position of the lateral upper lip/vermillion. (E) Repair at 6 months demonstrating normal form and function and excellent cosmesis. (Used with permission from Dr. Todd Holmes).
separately. (E) Repair at 9 months demonstrating mild asymmetry.
For defects near the vermillion, a standing tissue cone is removed superiorly and a
broad flap is advanced from the lateral lip and medial most cheek. The design includes an inferior base which parallels the vermillion border just a millimeter above it and extends lateral to the oral commissure, where a standing tissue cone is removed as the flap advances. The flap is elevated in the plane just above the orbicularis oris. When the nasofacial sulcus is reached, a reservoir of freely mobile tissue is tapped. The flap is thus freed of essentially all pivotal restraint. The flap should not be bulky and, in general, does not include any muscle fibers. The pedicle is from the superolateral aspect of the flap. Freed from all lip restraints, the flap may be advanced without distortion of the lateral vermillion. It is essential that all tension be directed in a horizontal plane. Substantial attention to detail is required to ensure appropriate positioning of the lateral lip to avoid any tension on or depression of the ipsilateral vermillion. If in doubt, it is better to slightly depress the oral commissure rather than elevate it, as slight depression is easier to correct in follow-up. In most cases, the strong musculature of the perioral region will reestablish the position of the mouth within several months such that prolonged positional distortion is rare, though every effort should be made to have a tension-free closure.
For defects closer to the nose, or for very large defects of the upper lip, a modified advancement flap includes an arciform standing tissue cone that extends up and around the nasal ala and alar crease. By extending the repair superiorly and around the ala, the entire medial cheek can be mobilized. Even extensive lip wounds can be suitably repaired in this manner. When the surgeon elevates such flaps, it is important to avoid transferring a deep, bulky flap onto the upper lip. The base of the flap is broad, and the blood supply is reliable. As such, a relatively thin flap may be advanced with confidence. Even appropriately thin upper lip advancements may pincushion for a period of several months, though as a rule they will eventuate in an aesthetic repair. Thicker flaps without adequate undermining, and those with improper sizing, will remain bulky and unsightly appearing as a finger of tissue seemingly placed onto the lip, and in these cases revision is needed.
All upper lip advancements have an impact on the nasolabial fold, and asymmetry is a consequence. The aesthetic compromise of an absent nasolabial fold is usually offset by repair of a more important location, namely the upper lip, but this expectation should be discussed with the patient prior to repair. If needed, the nasolabial fold may be recreated at a later date.

Figure 40-26. For modest wounds of the lip a vertical linear closure is an excellent repair. (A) A vertically oriented wound on the lip and a linear repair design for closure. (B) The closure is long and passes right through the vermillion border in order to avoid a pucker at the inferior margin. (C) Final result at 1 year with aesthetic repair.
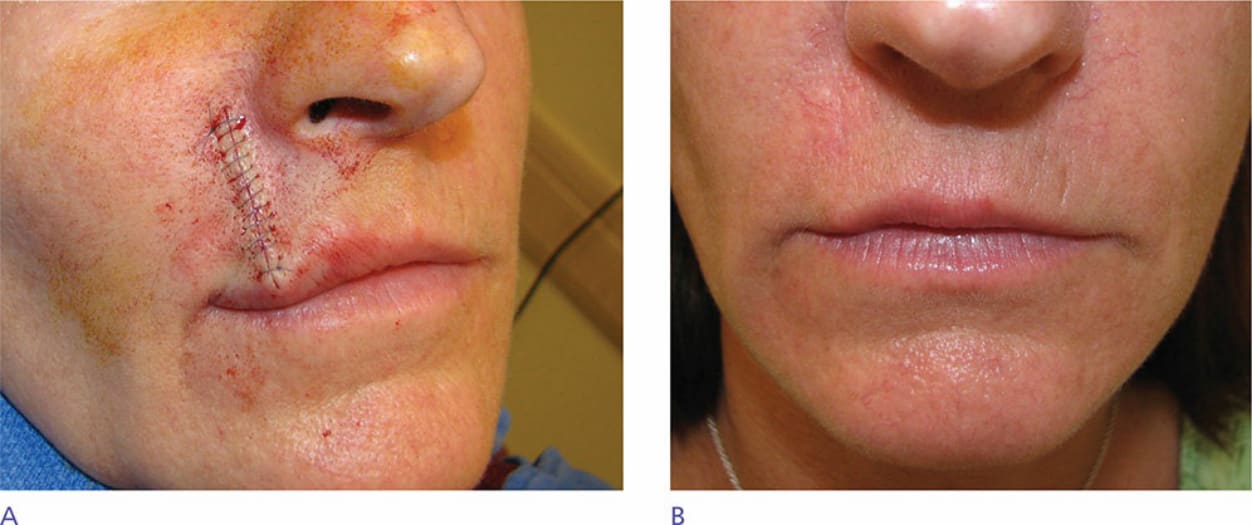
Figure 40-27. Fullness and puckering of the vermillion following a vertical linear repair. This is particularly problematic when smiling as it shows against the teeth. This can be avoided in most cases with proper planning and technique. (A) Immediate linear repair on the lip showing fullness and “bulldozing” of the upper lip vermillion. This can be avoided by removing the distal orbicularis oris band. (B) Photo at 6 months demonstrating resolution of most puckering, but still some fullness of the lip.

Figure 40-28. A slightly larger wound on the upper lip is repaired with a linear closure in which the distal/surface band of orbicularis oris is removed. (A) Operative wound. (B) The repair is performed in the potential space above the orbicularis musculature and is extended right through the vermillion border. The distal/surface band of orbicularis is excised and repaired as a “mini wedge.” (C) Immediate closure without pucker formation. (D) Aesthetic closure healing at 3 months.
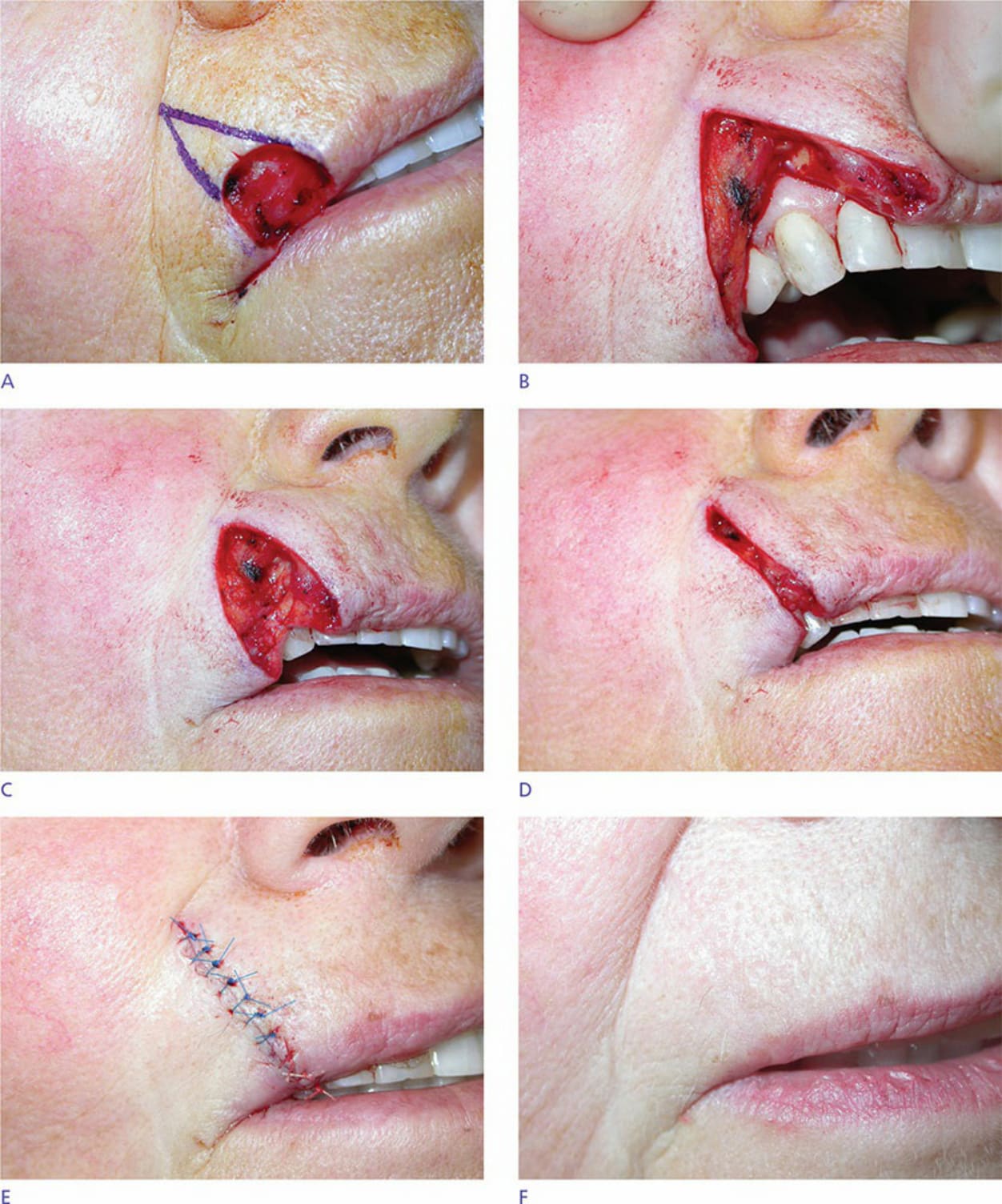
Figure 40-29. A modest wound of the lateral upper lip and vermillion is repaired with a wedge. (A) Operative wound and planned wedge. (B) A full-thickness excision has been accomplished. (C) The mucosa has been repaired. (D) The orbicularis oris has been reapproximated. (E) Repair at completion with careful matching of the vermillion border. (F) Repair at 6 months.

Figure 40-30. A modified wedge repair is performed as a partial-thickness closure without extension all the way to the gingival sulcus. (A) Operative wound and planned repair. (B) The wedge has been accomplished by excising the entire vermillion and all of the distal bands of the orbicularis oris. The labial artery has been ligated and transected. The upper bands of the orbicularis are preserved, and the wound edges are undermined free of the muscle. (C) The repair is closed by repairing the mucosa and the distal orbicularis band. (D) Immediate result without lip distortion. (E) Aesthetic repair at 6 months.

Figure 40-31. Figure and photos demonstrating a cheek advancement for a sizeable operative wound on the medial aspect of the lateral subunit. (A) Operative wound. A linear repair or wedge would distort the lip and displace the philtrum. A graft would be highly unaesthetic. (B) A large advancement flap is designed with crescentic standing tissue cones to be removed around the ala and lateral to the oral commissure. (C) The flap is elevated above orbicularis. This

Figure 40-32. In a modification of the prior repair, a large upper lip wound is repaired with a cheek advancement and a separate vermillion advancement (A) A large operative wound might be repaired with a lip wedge, but the patient is a tuba player and wishes to maintain his embouchure. (B) Advancement is designed to tap into laxity of the medial cheek. A crescentic standing tissue cone is delineated around the alar margin. (C) The flap is elevated out to and beneath the nasolabial fold. (D) The repair at completion. The vermillion has been undermined and advanced/rotated

Figure 40-33. A large defect of the left upper lip is repaired with a cheek advancement and a mucosal island pedicle flap. (A) Operative wound encompasses much of the lateral subunit and includes a mucosal defect. (B) The mucosal wound has been repaired with a mucosal island flap. (C) Advancement planned. (D) The flap has been advanced into place. (E) Final result at 1 year demonstrates normal lip contour. There was some tension on this repair, and the scars are visible and hypopigmented.