Partial repairs
Partial repairs
The figures and discussions included in Table 40-1 demonstrate that partial repairs of the lip can offer acceptable results with minimum morbidity and reduced cost (Fig. 40- 10). This is true even when the defect straddles the vermillion border. Patient selection,
of course, is of critical importance. Repairs can often be executed without significant extension or conversion to a fusiform shape, and no attempt to excise incipient standing cutaneous cones. Partial repairs can dramatically foreshorten the length of the repair, averting standing cutaneous cone formation over the perioral convexities.
The key to partial repairs is to tighten the sutures (buried and/or surface, at the surgeon’s discretion) just to the point where incipient standing cutaneous cone formation begins. With experience, the surgeon can know exactly how much cone formation will be exactly countered by the healing-process wound contraction. A flat scar of absolutely minimum length will result. In most cases, the surgeon should move up one suture diameter and leave sutures in place for roughly an extra week to prevent respreading of the wound with suture removal. In other words, as a rough approximation, if a linear closure at the site typically requires 6-0 suture removed at 10 days, the partial repair utilizes 5-0 suture for 2½ weeks. As the wound contracts, the suture typically becomes lax and irrelevant. Of course, one may elect no surface suture at all, tensioning the wound with only deep sutures.
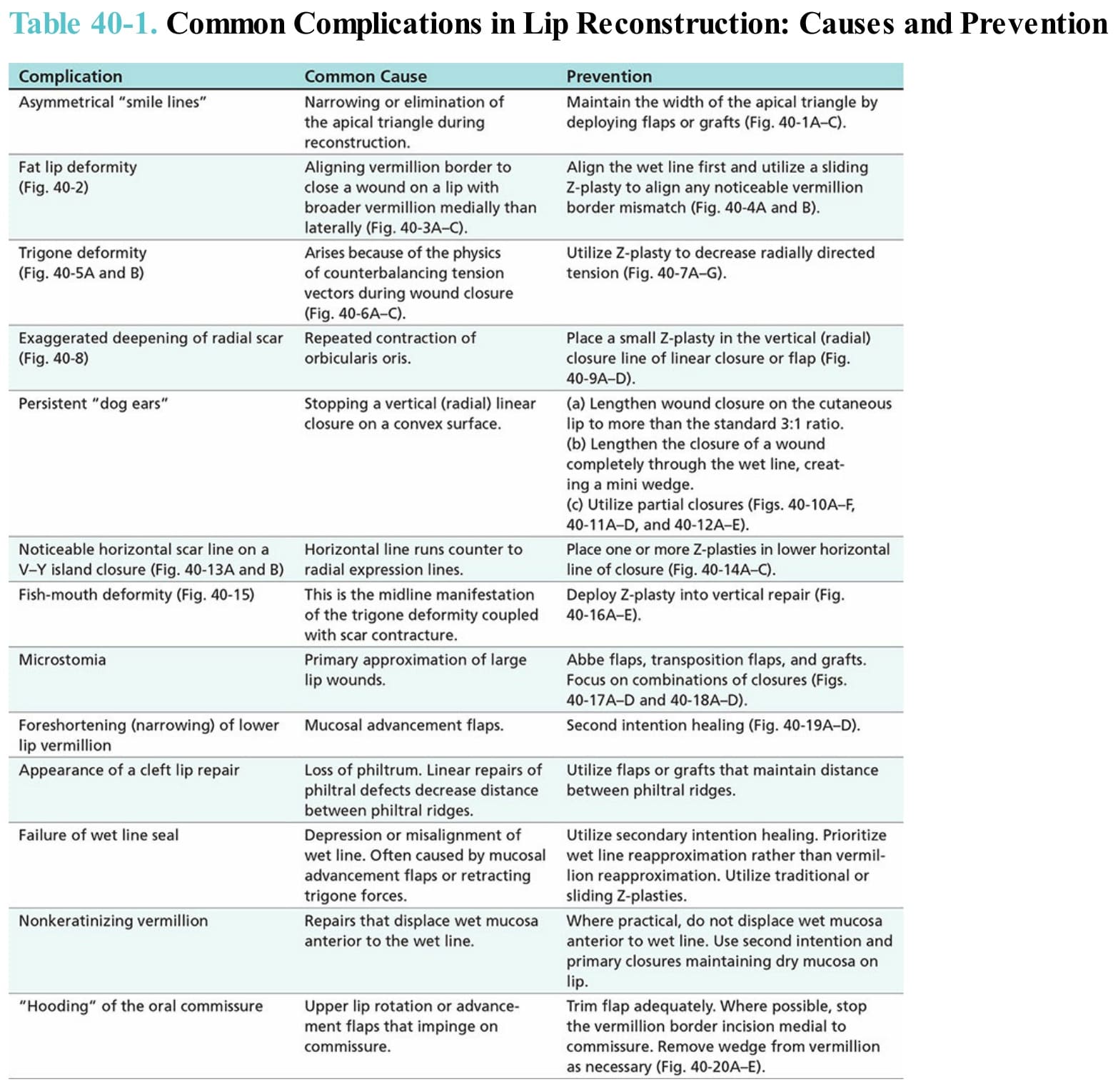
Table 40-1. Common Complications in Lip Reconstruction: Causes and Prevention