REPAIR-RELATED DEFORMITIES
REPAIR-RELATED DEFORMITIES
Any surgical wound of the lip can be repaired successfully in a variety of ways. By and large, the art of reconstructive surgery is the art of minimizing deformities. During reconstructive planning and execution, the foremost question in the surgeon’s mind must be, “How do I best serve this patient’s goals?” If those goals are best served by a reconstructive effort, the next most important question to ask oneself is, “How do I minimize noticeable deformity?” and not “How do I close this wound with XYZ closure?”
To develop the “deformity avoidance” mindset, the reconstructive surgeon must have a thorough understanding of how deformities arise during and after reconstruction. A mental catalog of possible deformities and their causes is more important to the reconstructive surgeon than the mental catalog of the repairs in the surgeon’s toolbox. Table 40-1 reviews some of the more salient deformities that the reconstructive surgeon should minimize or avoid altogether.
Figure 40-6 demonstrates why a trigone deformity develops. In an upper lip wound, for example, if the medial vermillion border is oriented horizontally, but the slope of the
lateral border is oblique, the original forces on the lip change when the surgeon approximates wound margins. A new upward force and a new medial force (defined by a single composite tension vector) now act on the wound’s lateral vermillion border. There is a concomitant two-component (lateral/downward) composite force now applied to the medial vermillion border.
When two forces act on a single point, that point will move along the net vector. Physics dictates that the movement continues until either (a) the original tension vectors are aligned at 180 degrees (i.e., the slope of the vermillion border is perfectly flat) or (b) the net tension vector along which the point moves is ultimately opposed by an equal and opposite tension vector.
In practice, “b” is the only scenario that happens if one sutures two sides of a wound whose opposing medial and lateral vermillion borders are not horizontally co-linear. In this case, a “corner” will form along the vermillion border at the physical point where there is an equalization of the three tension vectors. If the angle of that “corner” is broad, the effect is minimally noticeable. As forces increase, however, the angle becomes more acute; there will be a progressively more noticeable “corner” at the vermillion border.
This is termed a “trigone deformity.” It does not occur in suturing the wound in a thin, flat lip, as there is no upward or downward force on the reconjoined vermillion border.
A trigone deformity is an inevitable outcome of the physics of tissue movement in a lip with vermillion border of changing slope. It can accompany a fat lip deformity, though this does not occur consistently. While the trigone deformity relates to the changing slope of the vermillion border, the fat lip deformity relates to the changing cross-sectional arc of curvature.
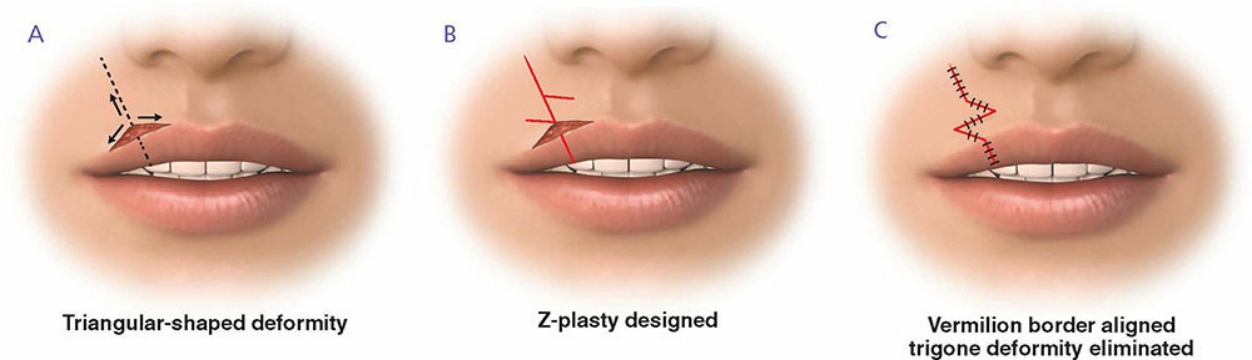
Figure 40-6. (A) When the wound is sutured, tension vectors create forces that pull the vermillion border into a triangular deformity. (B) Z-plasty designed to correct the incipient trigone deformity at the initial closure. (C) With Zplasty execution, the vermillion border is compelled to follow a smoothly continuous curve.
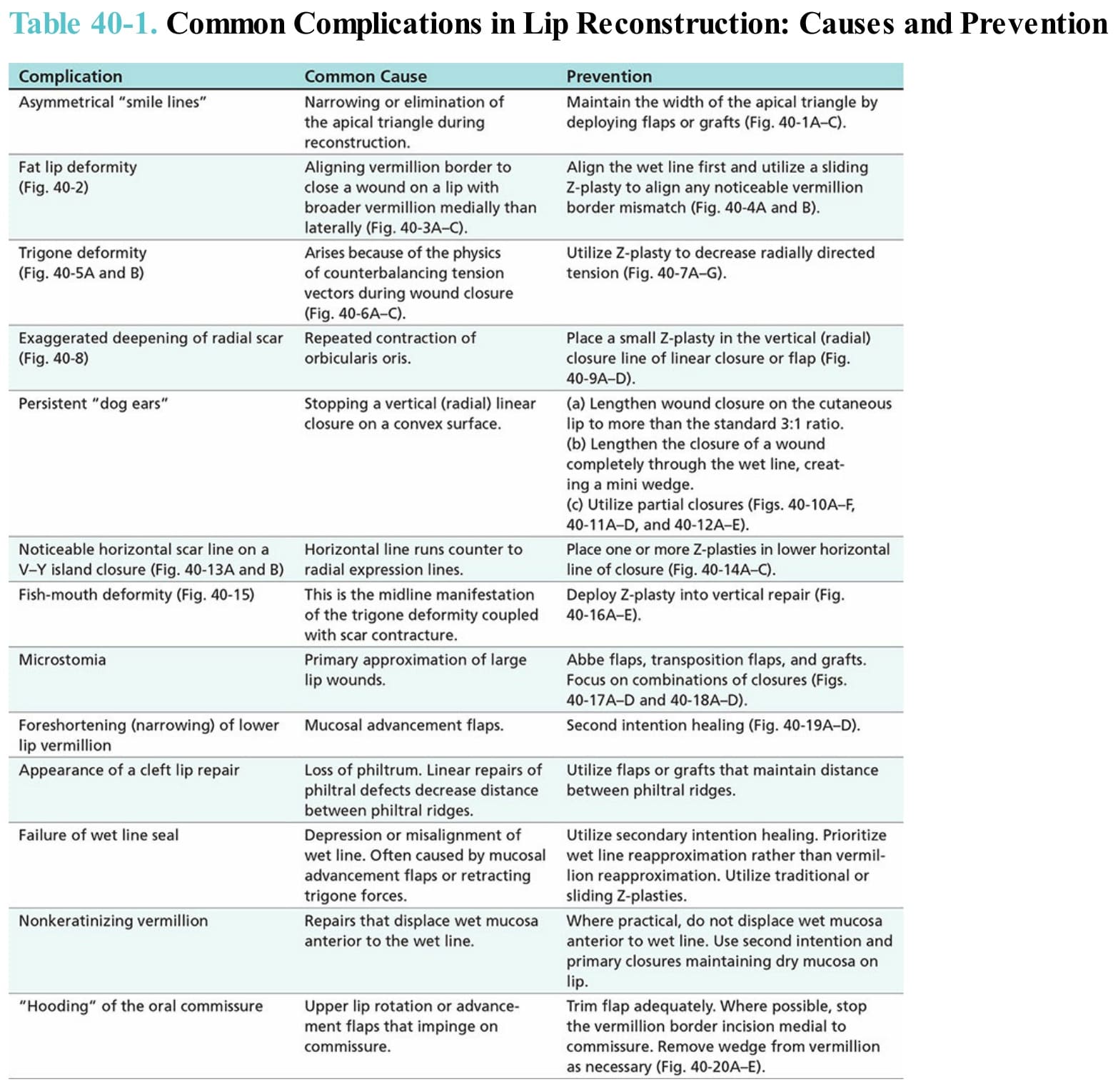
Table 40-1. Common Complications in Lip Reconstruction: Causes and Prevention