BIOANATOMY AND BIOMECHANICS
BIOANATOMY AND BIOMECHANICS
Perceptually, the upper lip is composed of multiple cosmetic subunits (Fig. 40-21).1 The central philtral subunit is bounded on either side by the philtral ridges, the medial borders of the lateral subunits. The lateral subunits of the upper lip are bounded inferiorly by the vermillion, medially by the philtral ridges, superiorly by the bases of the alae and columella, and laterally by the nasolabial fold. The apical triangle, sometimes called the isthmus, is the small triangular extension of the lip which lies lateral to the ala and medial to the superior most nasolabial fold. While small in size, it provides a recognizable delineation between the lip, nose, and cheek; it should be maintained as an aesthetic marker whenever feasible.
The inner surface of the lip is the oral mucosa. The wet mucosa becomes vermillion as it exits the oral aperture and forms the red lip. External to the wet line, the vermillion surface represents “dry mucosa.” The keratinizing dry mucosa differs structurally from nonkeratinizing wet mucosa. For this reason, skin grafts of wet mucosa onto the dry mucosa of the vermillion do not mature into dry mucosa. Utilizing wet mucosa to repair the vermillion surface external to the wet line often yields suboptimal results.
Beneath the mucosa is a submucosal layer rich in minor salivary glands. The vermillion itself lies directly on a circumoral band of orbicularis oris and the underlying musculature has rich vascular supply. This leads to the red color of the lips. The structural bulk of the lip is composed of the orbicularis oris, which forms circumferential rings and gives the lips their shape, definition, and function.
The facial nerve provides motor innervation for the perioral musculature via its zygomatic, buccal, marginal mandibular, and cervical branches. These nerves are highly anastomosed and deeply seated. Therefore, neural injury leading to a functional impairment of perioral function is rare, with the one exception being damage to the marginal mandibular nerve as it passes along the mandible. The infraorbital nerve provides sensory function to the upper lip, and the mental nerve innervates the lower lip
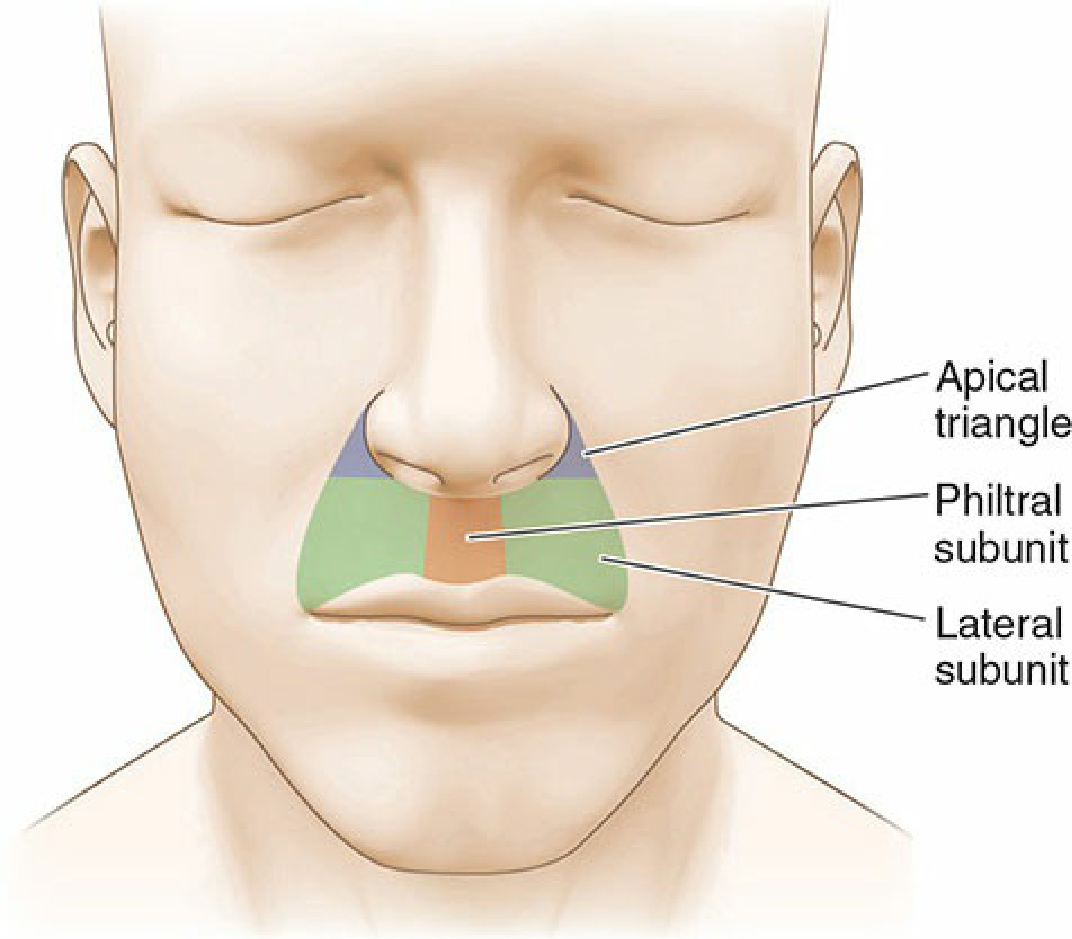
Figure 40-21. Lip subunits: The upper lip is divided into a philtral subunit and two lateral subunits. The lateral subunits each contains an apical or “sacred” triangle lateral to the nasal ala. Maintaining the integrity of the philtrum, apical triangle, and nasolabial folds are goals of upper lip reconstruction.
(Fig. 40-22).
(Fig. 40-22).
Anesthesia of the lip is readily achieved by nerve block (see Chapter 12). The upper and lower lip each receive a large branch from the facial artery as it ascends toward the alar crease (Fig. 40-23). The arteries run in the submucosa and become tortuous with age. They give off many perforators and branches, anastomosing at the midline.
The junction of the vermillion and the cutaneous lip is a bright, clear line in younger adults. A thin, elevated, well-defined band of pale glabrous skin (the white line) marks the border with the cutaneous lip. With age, this definition fades progressively until the vermillion border is no longer a line but a vaguely defined zone up to 4 mm wide where vermillion blends in a continuum with the cutaneous lip. The reconstructive surgeon must remain keenly aware of the width of this vermillion/cutaneous transition. If the patient has a white line, the repair must be meticulous, reapproximating the white line on apposing wound margins. If the vermillion/cutaneous transition is a wider “zone” of transition, the vermillion alignment is less critical. The observing eye will not notice the repair scar as long as the vermillion “border” on either side of the repair falls within the vaguely defined “zone.”
The youthful lip often has a prominent philtrum, and the vermillion border of the upper lip is crisp and voluminous. The nasolabial folds are not well developed in youth. Instead they are soft, minimally depressed inclinations. With age, the upper lip flattens, the philtrum is less prominent, and the vermillion border is less defined. The nasolabial folds become fixed and sharply recessed, clearly defining the lateral margin of the upper lip (Fig. 40-24).
There is tremendous variation in the shape of the perioral region, and this has an impact on reconstruction (Fig. 40-25). Some individuals have a small oral opening, while others have a broad, wide mouth. The upper lip may be high and arched, or low and flat. The distance from the columella to the vermillion varies dramatically from person to person, as does the span from commissure to commissure. While most younger individuals have a prominent philtrum, in some it is minimal even in youth. In some older individuals there is no residual philtrum at all. Such variation impacts operative reconstruction, as what may be a simple repair in some individuals can be a challenge in others.
This chapter focuses on the aesthetic and functional repair of modest wounds of the upper and lower lip. A storied history of reconstruction of the lip for large wounds dates to the late 1500s and involves some of the historically great reconstructive surgeons. In recent decades, dermatologic surgeons have greatly expanded the available repertoire of sophisticated reconstructions. While generally beyond the scope of this text, the artistry and geometry involved in the history of extensive wound lip reconstruction are well worth examining.2
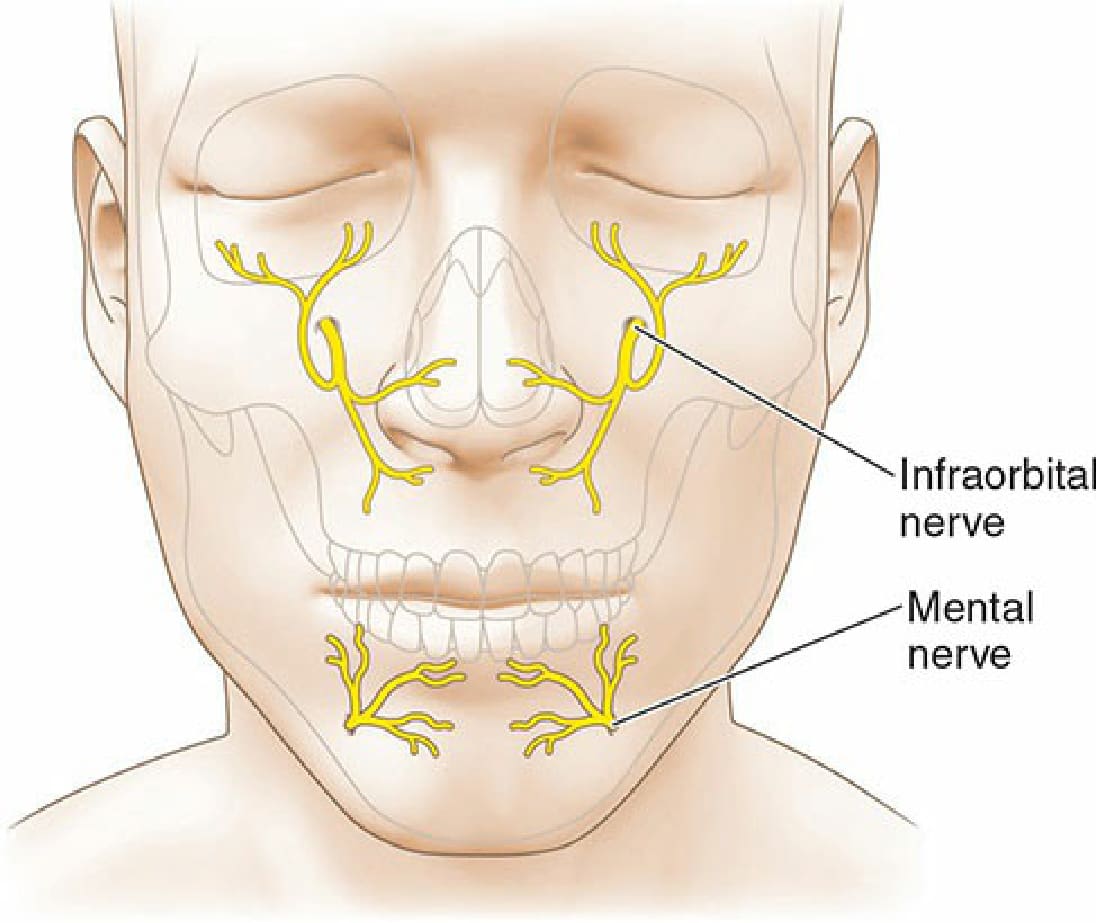
Figure 40-22. Sensory innervation of the perioral region. The upper lip is innervated by the infraorbital nerve and the lower lip is innervated by the mental nerve. The lateral commissures receive sensory input from the cervical nerves and require separate local anesthetic.
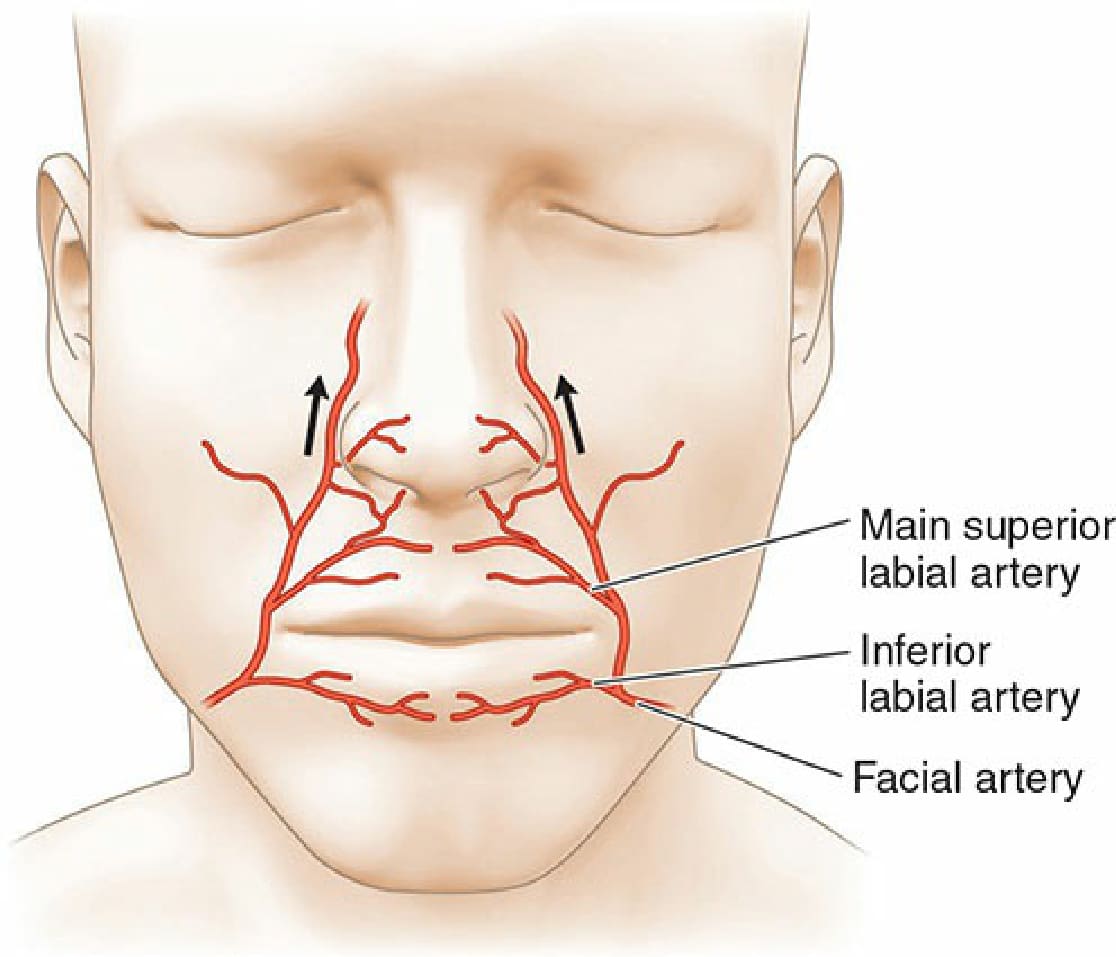
Figure 40-23. Vasculature of the perioral region. The upper and lower lips are richly supplied by large labial branches of the facial artery. The labial branches are tortuous with age and run on the submucosal side of the orbicularis oris.

Figure 40-24. Variation in the lip with age. (A) Lips of a 25-year-old woman. The vermillion is full and sharply defined. The philtrum is elevated and distinct. Repairs may be noticeable, even if the scar line is fine and sharp. (B) Lips of a 45-year-old woman. The vermillion has lost some volume. The philtrum has lost some elevation and is less distinct. A few vertical lines have formed. (C) Lips of a 65-year-old woman. Volume loss and loss of the philtrum are more advanced and vertical rhytides are more pronounced. Repairs are often less visible.
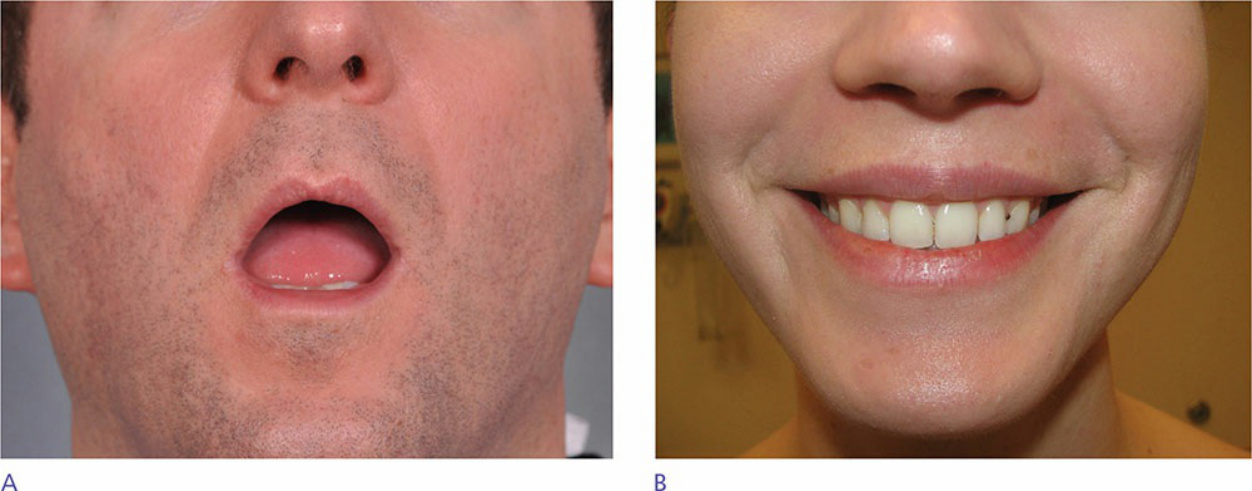
Figure 40-25. Variations in size and configuration of the mouth/lips. (A) Small oral aperture. Loss of any substantial component of the oral diameter may lead to relative microstomia. (B) A broad upper and lower lip make reconstruction easier in the event of a sizeable defect.