Lips
Lips
INTRODUCTION
The lips and perioral region represent a critical region both aesthetically and functionally. They are central to facial expression, are sensory organs for food and personal contact, and provide oral competence at rest and during mastication. The lips also have rich vasculature and sensory innervation.
The perioral region is bounded by the nasolabial folds laterally and superiorly, and by the mental crease of the chin inferiorly. The lips are suspended only by muscles and the fibrous tissues of the modiolus at each oral commissure. Therefore, the lips and the oral commissures represent mobile free margins. Reconstruction of the perioral region requires meticulous planning to direct tension in appropriate vectors. Retraction of the upper lip margin creates the appearance of a hair lip. Midline retraction may simulate a cleft lip repair. Distortion of the lateral oral commissure can lead either to drooling or a permanent sneer. Depression and/or eversion of the lower lip may lead to a loss of oral competence. Table 40-1 reviews many of the complications unique to lip reconstruction (Figs. 40-1 through 40-20).

Figure 40-1. (A) Wound involving entire apical triangle. The subalar upper lip is an especially effective donor site to reconstruct the apical triangle. (B) Flap in position. (C) Appearance at suture removal. Apical triangle preserved.

Figure 40-2. Aligning the wet line after the white line (vermillion border) can result in a fat lip deformity.

Figure 40-3. (A) Wet line step-off when vermillion border is aligned as first step in reconstruction. (B) Aligning the wet line (instead of the vermillion border) results in a step-off at the vermillion border. (C) A sliding Z-plasty restores vermillion alignment while the wet line prioritized closure averts a fat lip deformity. (Reproduced with permission from Wentzell JM1, Lund JJ: Z-plasty innovations in vertical lip reconstructions, Dermatol Surg. 2011 Nov;37(11):1646– 1662).
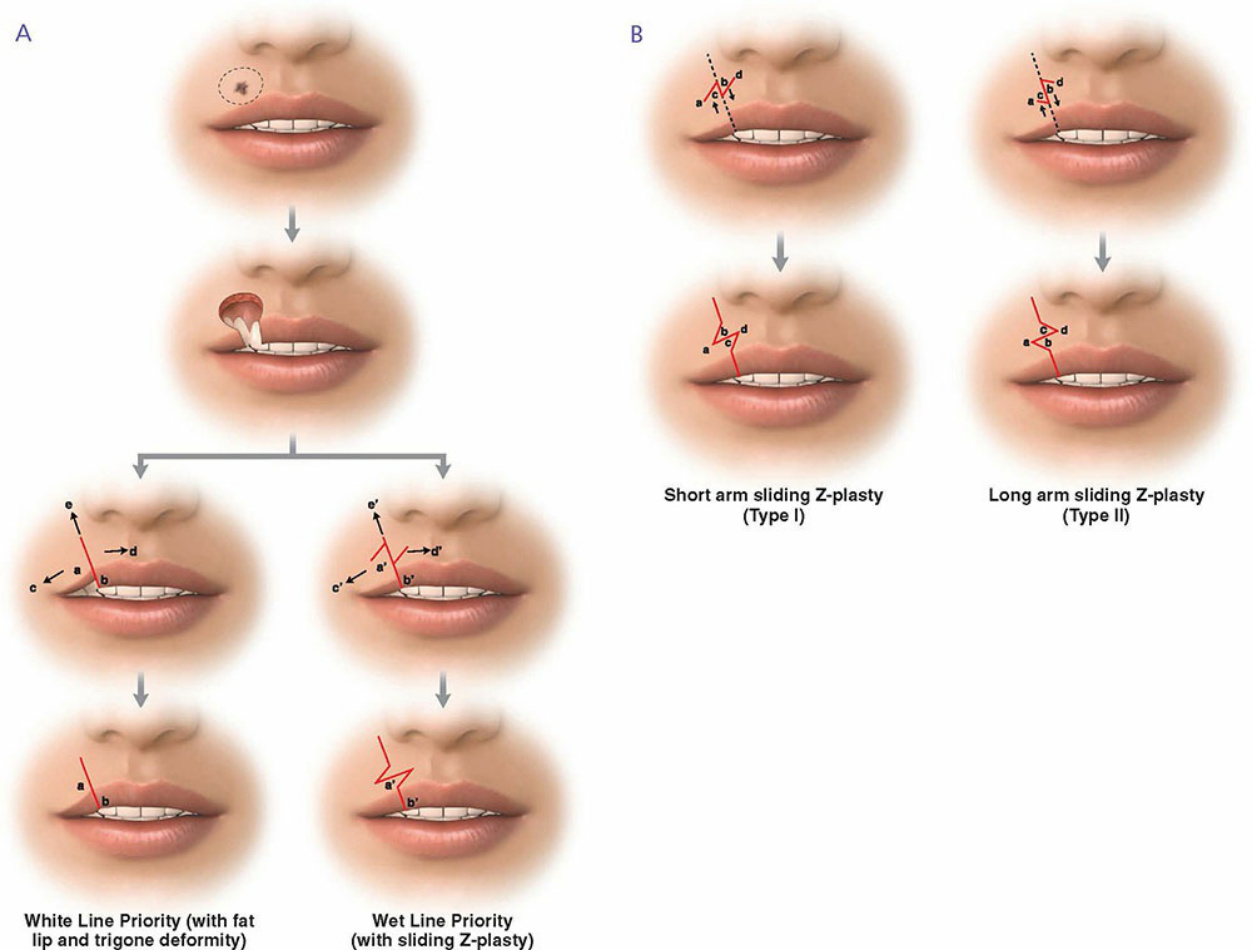
Figure 40-4. (A) In a white line prioritized lip alignment, a wet line step-off and trigone deformity can occur under common conditions. A fat lip deformity can occur with correction of the wet line step-off. In a wet line prioritized alignment, a sliding Z-plasty corrects the white line misalignment. In addition, tension vectors c’, d’, and e’ are reduced relative to tension vectors c, d, and e, reducing the source of the trigone deformity. (B) A Z-plasty will “slide” one side relative to the other side if the central limb is not the same length as the side limbs. In practice, the surgeon may elect a short central arm or a long central arm, but the Z-plasty configuration must change to achieve the same correction, depending on whether the central limb is short or long.

Figure 40-5. (A) Rotation flap creating trigone deformity of the vermillion border. (B) Trigone deformities and fat lip deformities are evident at suture removal and do not improve with time. (Reproduced with permission from Wentzell JM1, Lund JJ: Z-plasty innovations in vertical lip reconstructions, Dermatol Surg. 2011 Nov;37(11):1646–1662).
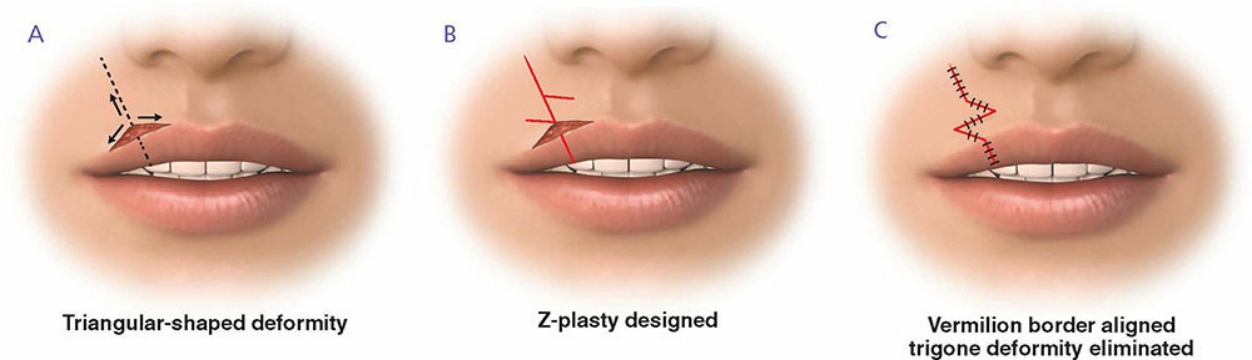
Figure 40-6. (A) When the wound is sutured, tension vectors create forces that pull the vermillion border into a triangular deformity. (B) Z-plasty designed to correct the incipient trigone deformity at the initial closure. (C) With Zplasty execution, the vermillion border is compelled to follow a smoothly continuous curve.

Figure 40-7. (A) Large upper lip defect. (B) and (C) Vertical revision outlined and initiated. (D) In this case, approximation of wet line does not result in vertical misalignment of vermillion border because the lip’s cross-sectional arc of curvature is the same medially and laterally. A sliding Z-plasty is not necessary. However, wound closure completion at this point would result in a “corner” or trigone deformity at the border. (E) and (F) A traditional Z-plasty compels the vermillion border to follow a smoothly continuous line. (G) Long-term result without trigone deformity. (Reproduced with permission from Wentzell JM1, Lund JJ: Z-plasty innovations in vertical lip reconstructions, Dermatol Surg. 2011 Nov;37(11):1646–1662).

Figure 40-8. Exaggerated creasing of right upper lip scar due to repeated muscular contraction. (Reproduced with permission from Wentzell JM1, Lund JJ: Z-plasty innovations in vertical lip reconstructions, Dermatol Surg. 2011 Nov;37(11):1646–1662).
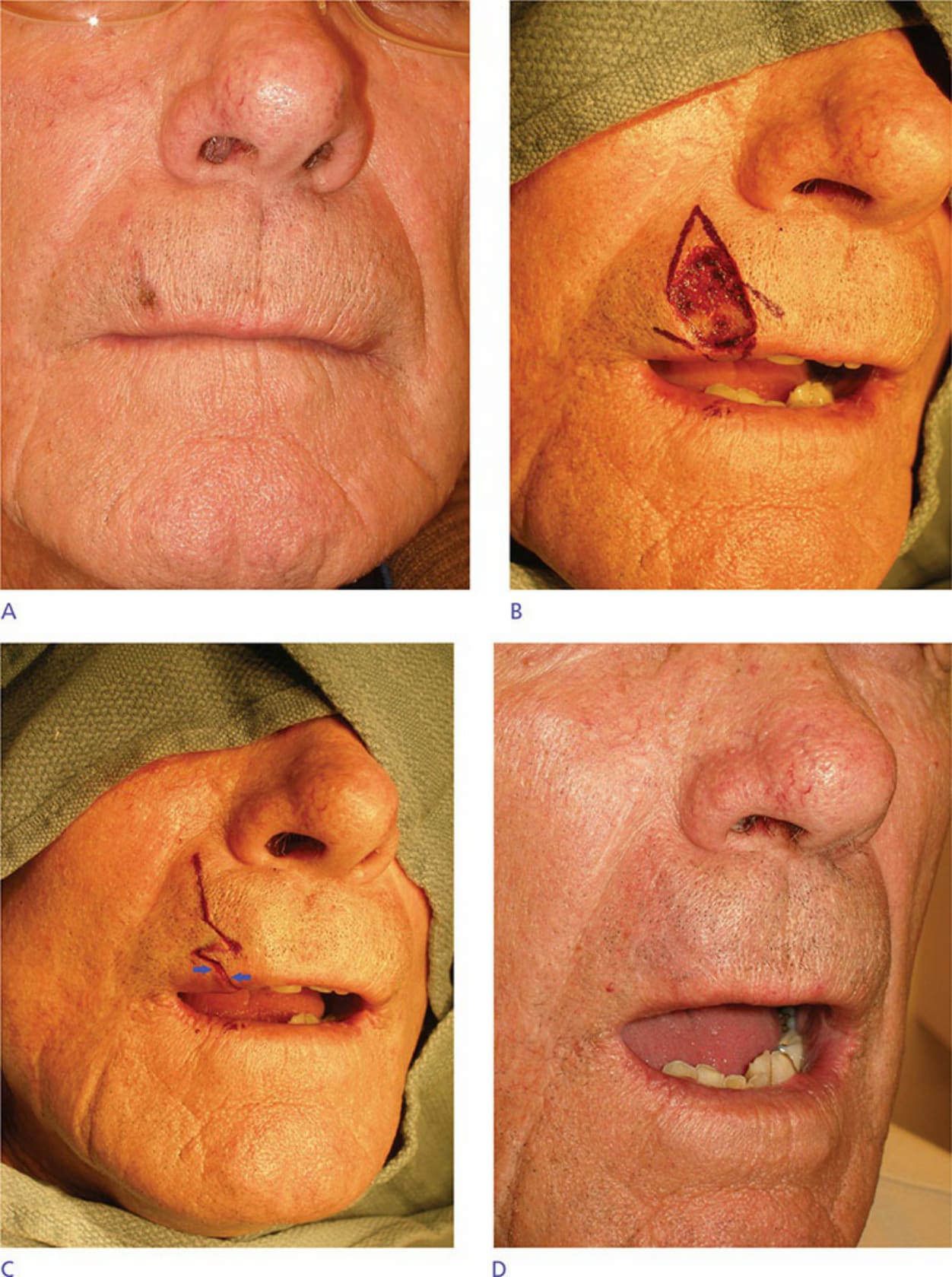
Figure 40-9. (A) Vague vermillion border zone. (B) Defect with Z-plasty outlined. (C) Z-plasty executed. Arrows demonstrate misalignment of vermillion border. (D) Final outcome. Misaligned border is imperceptible. Horizontal limb of Z-plasty acts as a reinforcing strut to counter contractile forces that cause exaggerated creasing. (Reproduced with permission from Wentzell JM1, Lund JJ: Z-plasty innovations in vertical lip reconstructions, Dermatol Surg. 2011 Nov;37(11):1646–1662).
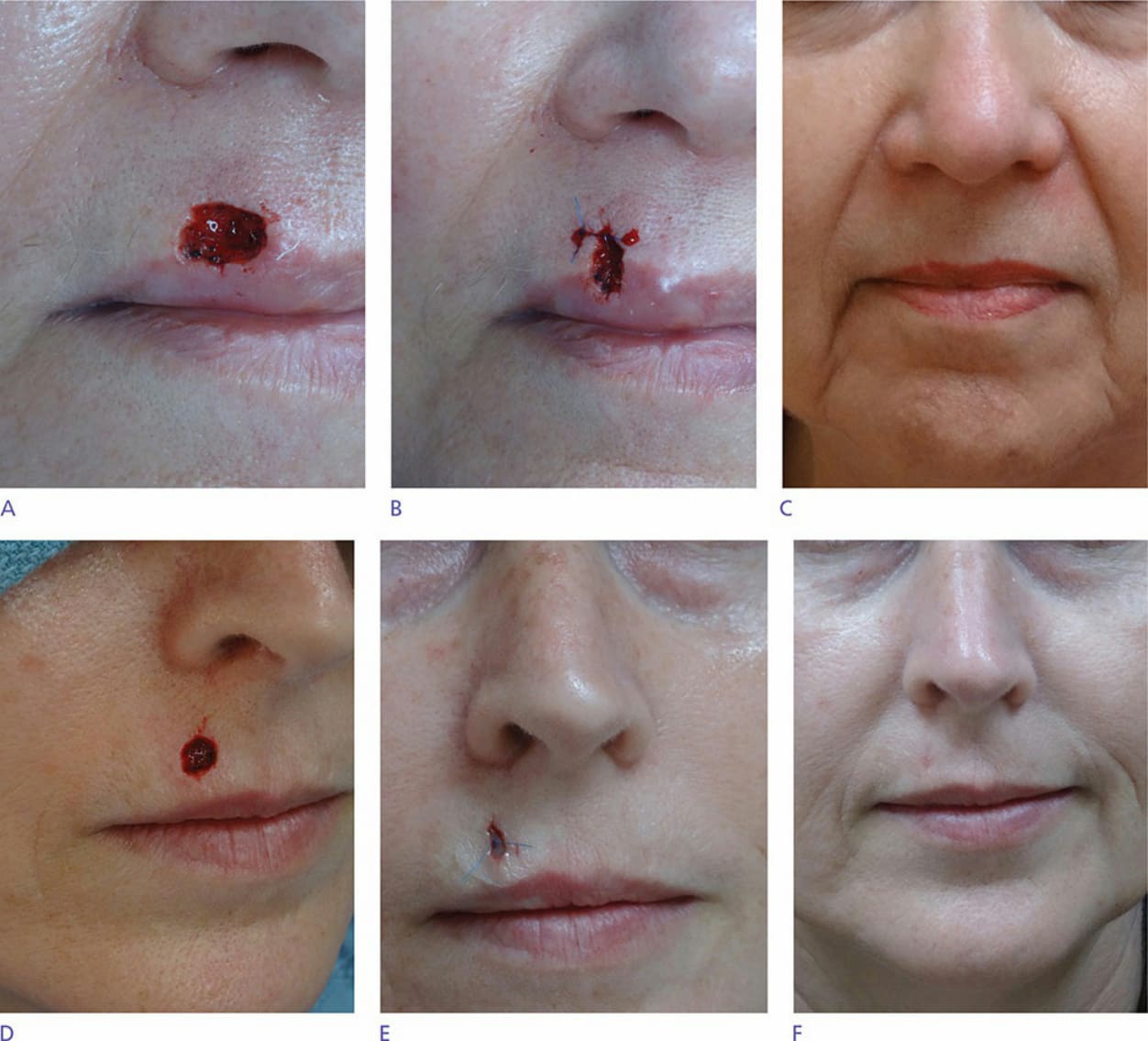
Figure 40-10. (A) Vermillion border defect. (B) Partial closure just deflecting superior and inferior wound margins to counteract wound contraction forces. (C) Long-term result. (D) Cutaneous lip defect. Complete 3:1 closure would result in inferior dog ear necessitating wound extension through wet line. (E) Wound closed just to the point where superior and inferior wound margin deflection will neutralize opposing contractile forces while the wound heals. (F) Short-term result.
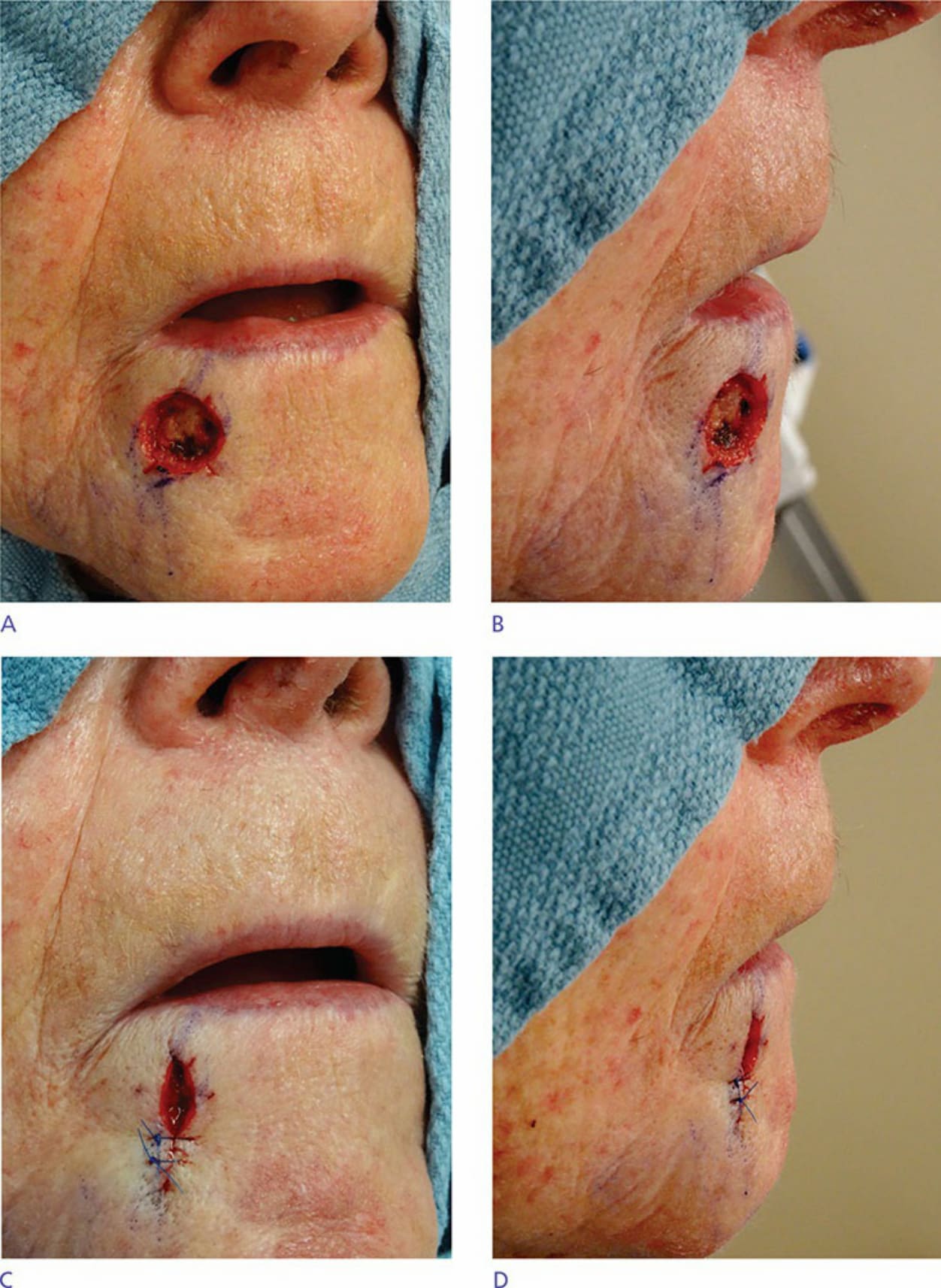
Figure 40-11. (A) Typical lower lip defect. (B) Superior aspect of the defect just approaches the apex of convexity. Traditional 3:1 linear closure would create a dog ear deformity at the vermillion or require a vermillion wedge. (C) Closed wound within its own length, compressing the superior aspect side-to-side with deep sutures only. (D) Superior aspect closed just to the point of incipient cone formation; this just counters contractile forces of healing wound to prevent downward contraction of vermillion border.
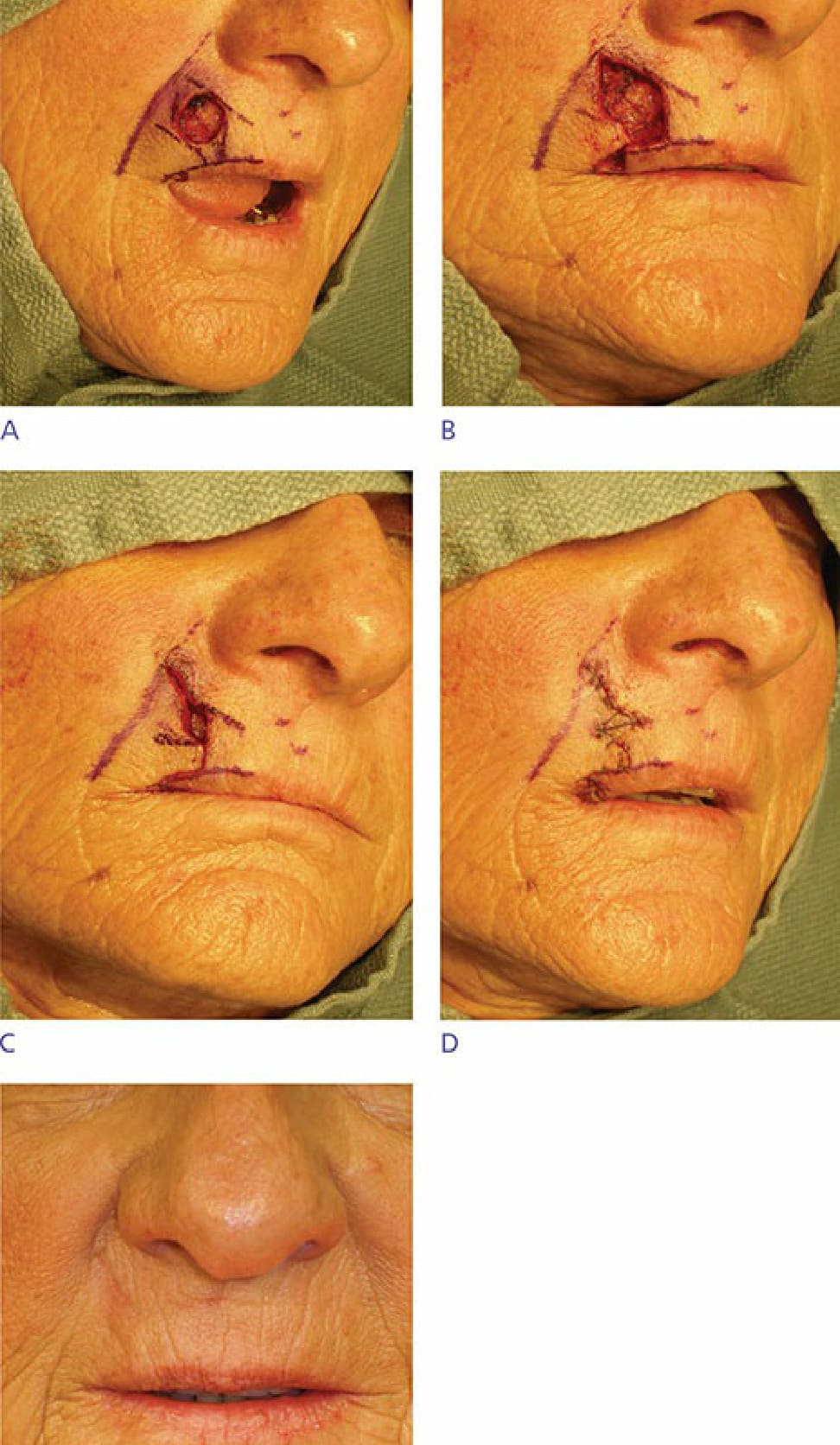
Figure 40-12. (A) Moderately sized defect on the upper lip with advancement flap designed along the vermilion border. (B) Standing cone and back cut removed and flap incised. (C) Flap brought into position. Note the residual central defect with Z-plasty marked out. (D) Final closure after central Z-plasty. (E) Long-term follow-up.

Figure 40-13. (A) Small squamous cell carcinoma of upper lip. (B) Inappropriately large repair with pronounced horizontal limb on V–Y island pedicle advancement flap.

Figure 40-14. (A) Larger cancer excision site compared to Figure 40-13. (B) Appropriately sized V–Y island pedicle marked for Z-plasty. (C) Executed Z-plasty on lower horizontal line will camouflage scar. Two or more Z-plasties can be deployed as necessary.

Figure 40-15. Fish-mouth deformities arise due to the same force vectors as trigone deformities. Scar contracture often contributes.
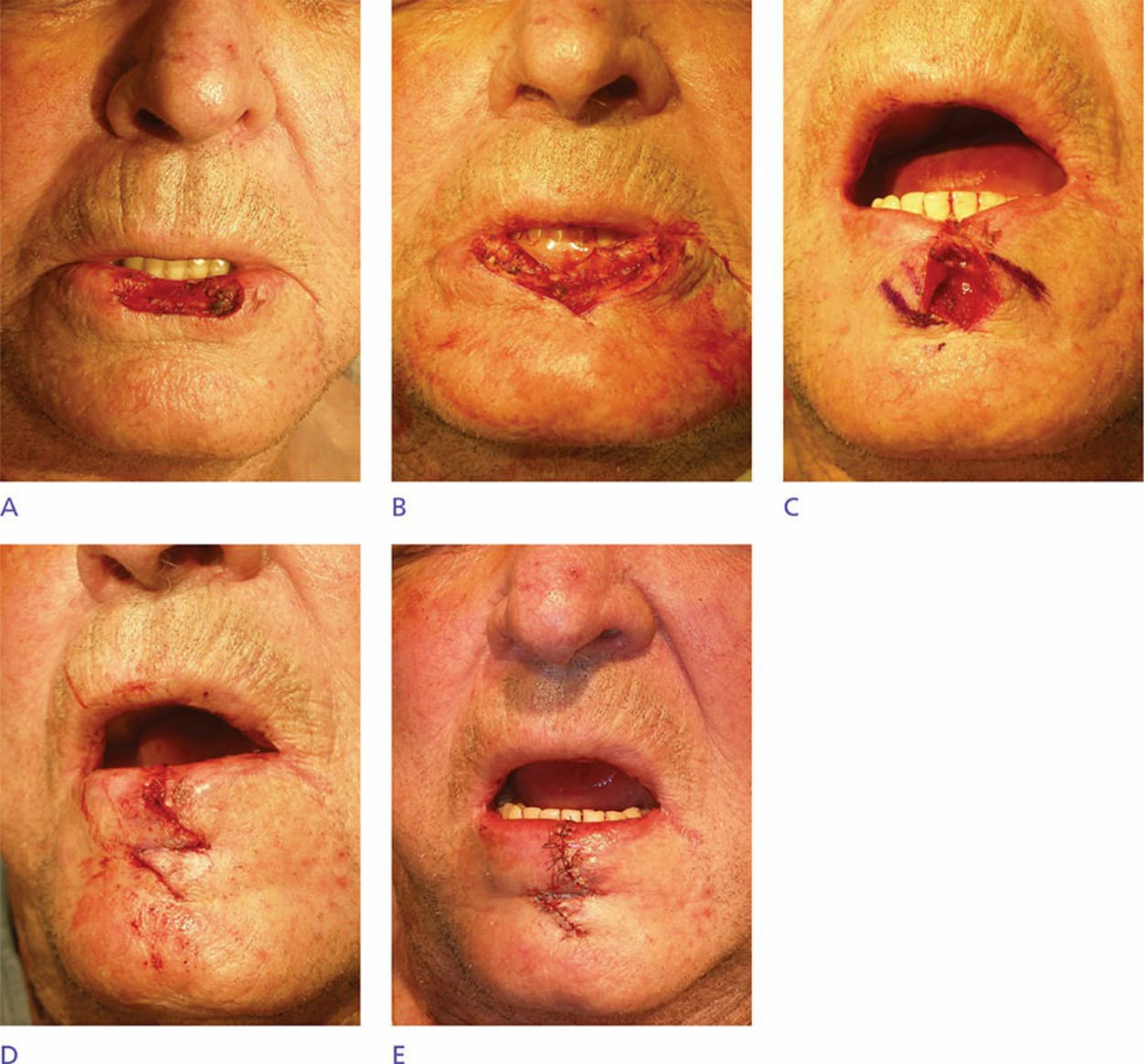
Figure 40-16. (A) Broad defect into muscularis. (B) Defect appearance after wedge excision. (C) Approximation with incipient fish-mouth deformity. (D) Z-plasty corrects fish-mouth deformity. (E) Final horizontal arm of Z-plasty in labial-mental sulcus.
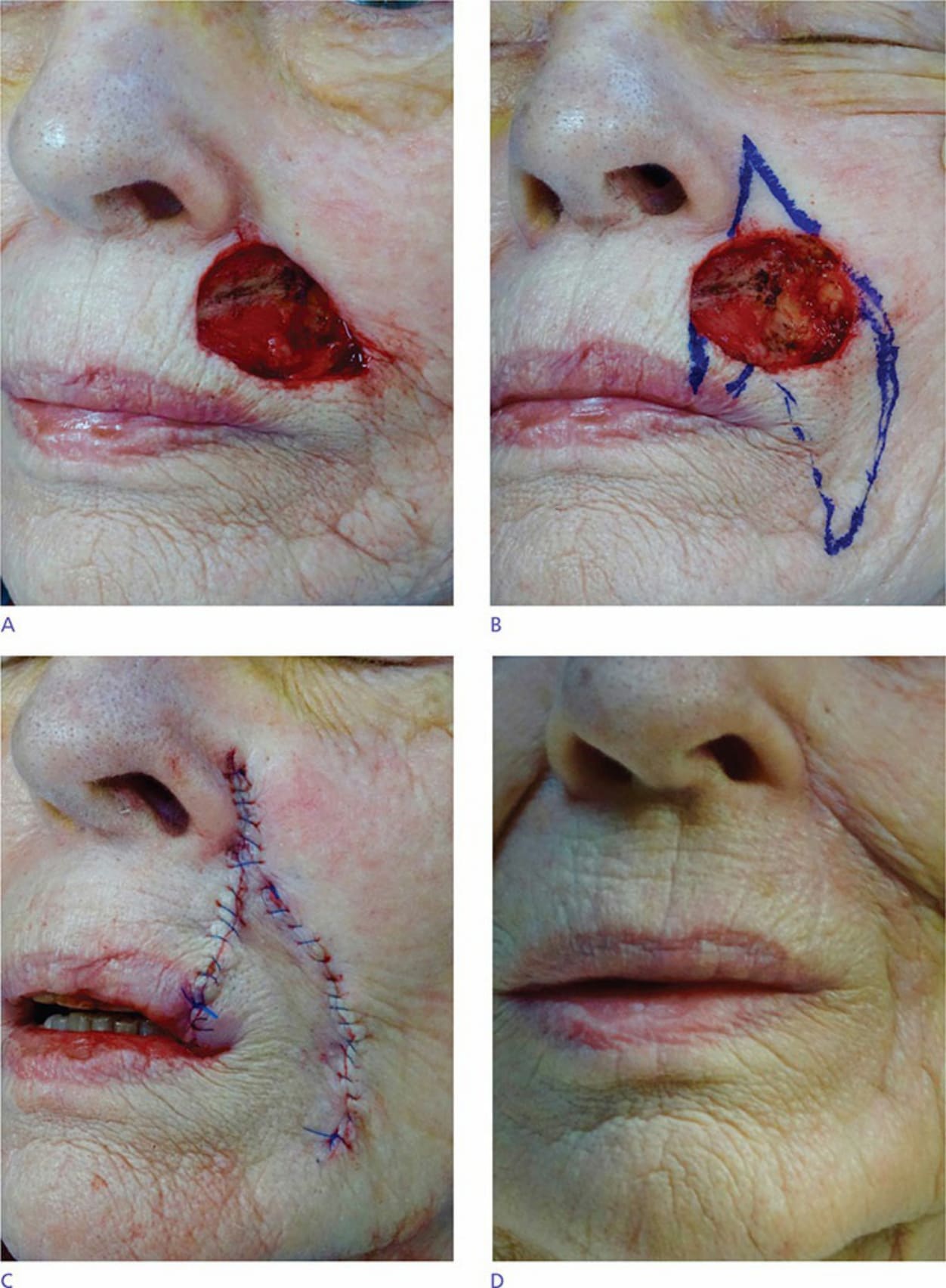
Figure 40-17. (A) Large, deep upper lip defect. (B) Design of combined rotation flap and wedge. Either closure alone would cause significant distortion or possible microstomia. (C) Final closure. (D) Long-term result.
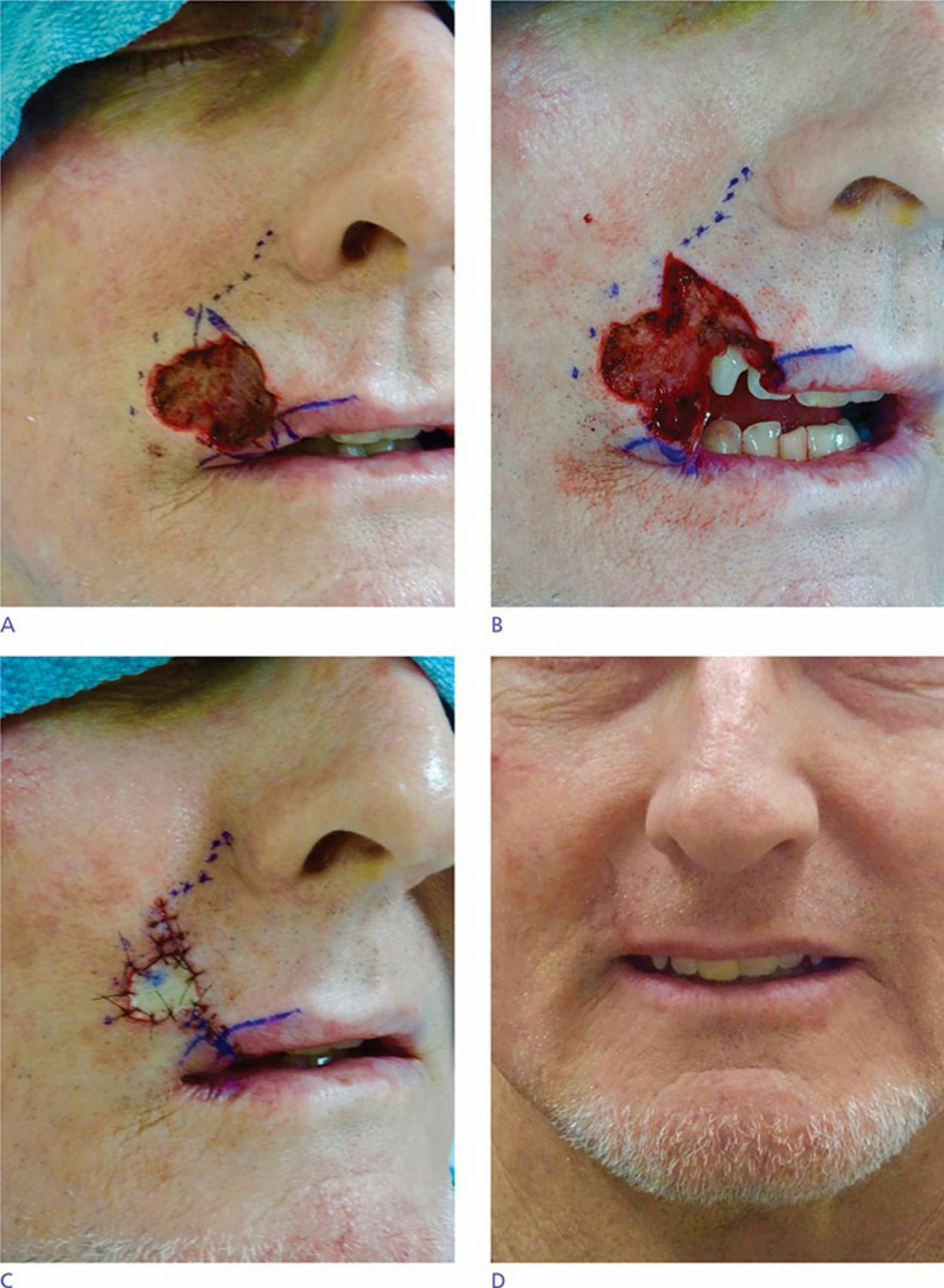
Figure 40-18. (A) Broad defect of lateral lip in youthful face equal to 60% of total width from commissure to midupper lip. (B) Medial wedge combined with (C) small lateral graft derived from hair-bearing submental neck crease. (D) Short-term result amenable to dermabrasion. A single flap or graft or wedge would cause much greater distortion and possible microstomia.

Figure 40-19. (A) Defects extending to muscularis. (B) Final outcome of second intention healing. (C) Two weeks after extensive excision to muscularis. (D) Final outcome with second intention healing. In many cases, second intention healing provides a superior result even for excisions of the entire lower lip, and even those involving muscularis or extending to the cutaneous lip.
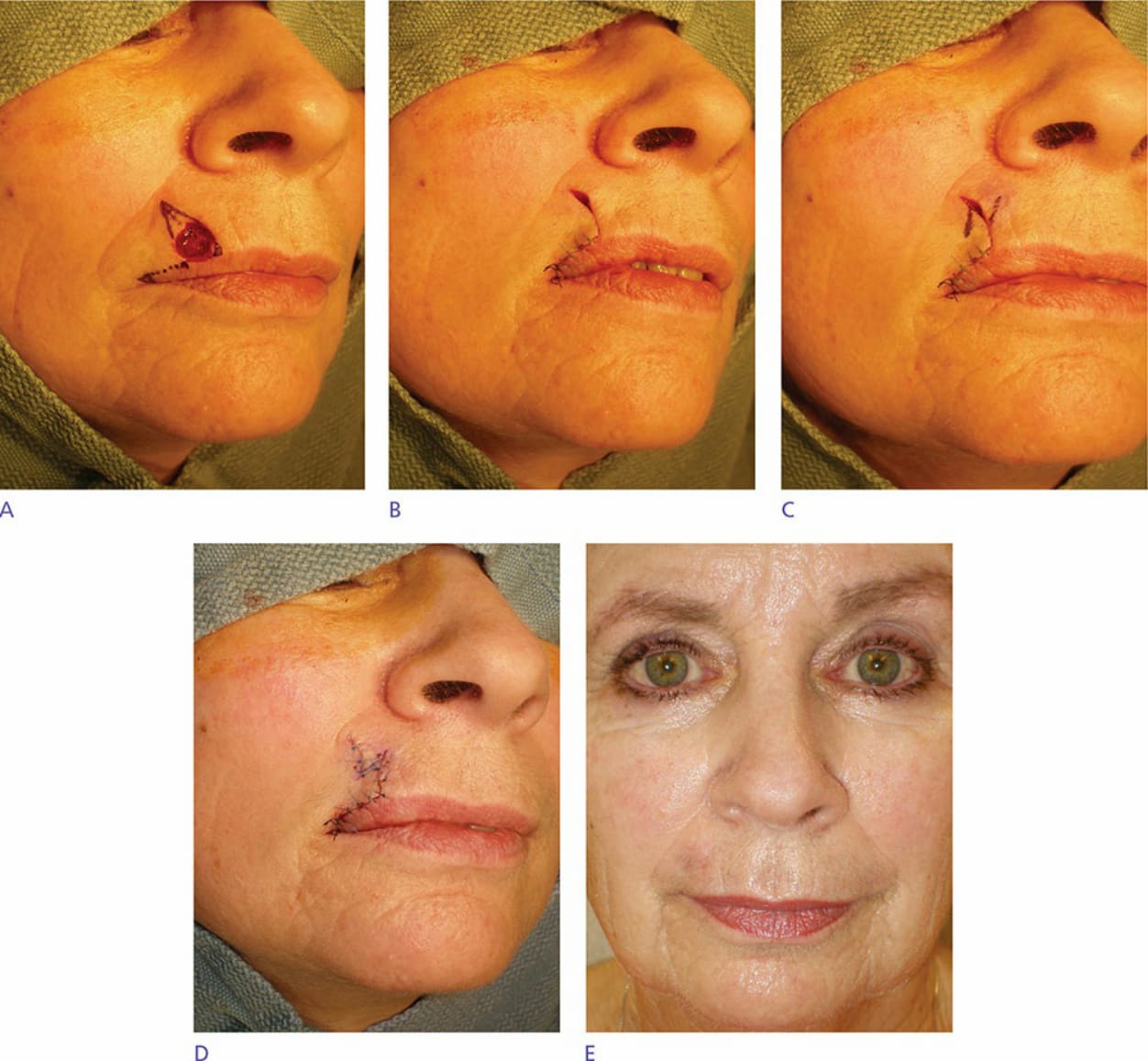
Figure 40-20. (A) Rotation flap designed with lateral vermillion wedge to prevent hooding. (B) Flap in position. (C) Z-plasty designed. (D) Flap fully executed. (E) Long-term result. No lateral hooding is seen.
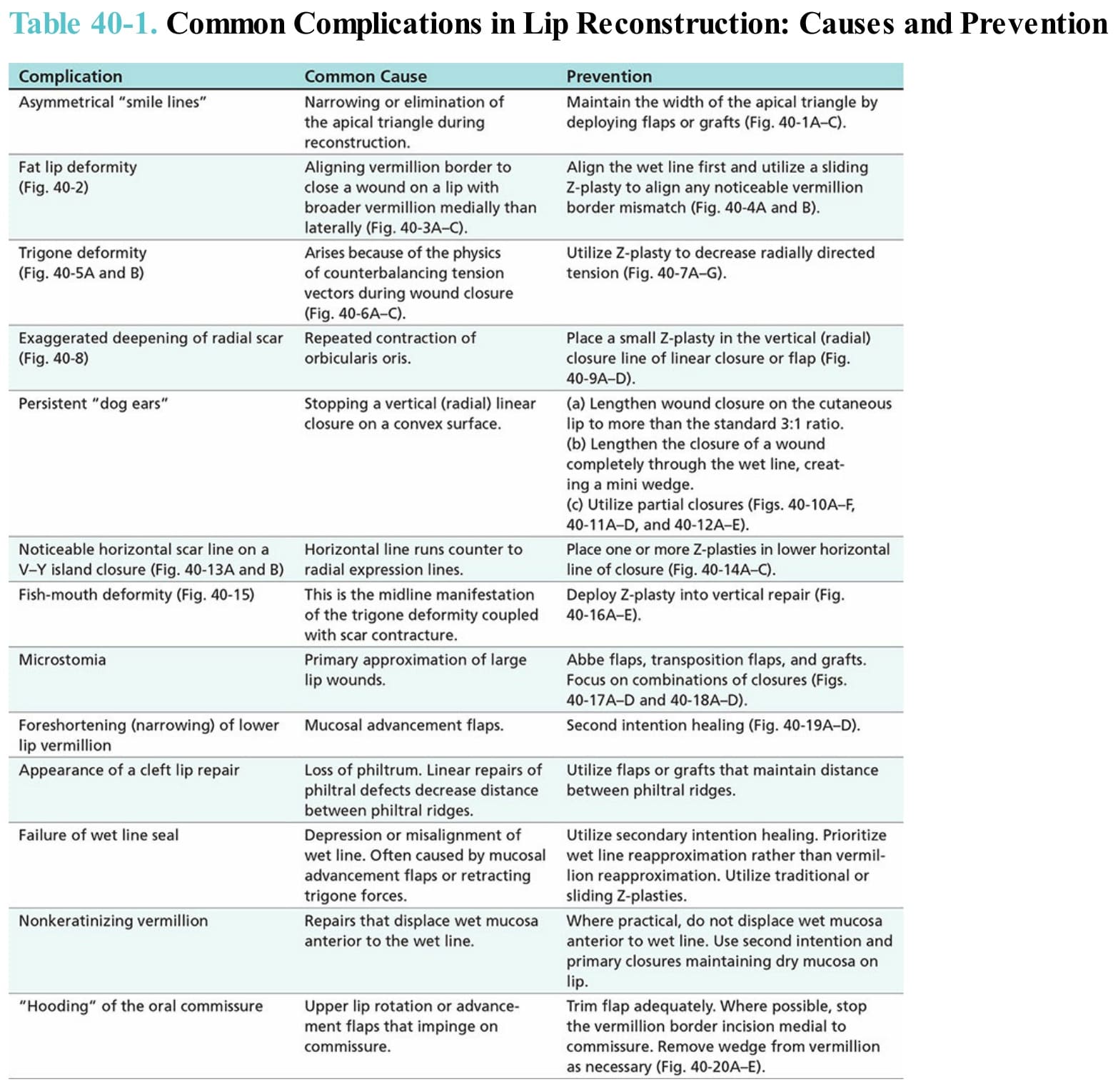
Table 40-1. Common Complications in Lip Reconstruction: Causes and Prevention