Transposition Flaps
Transposition Flaps
Transposition flaps avoid distortion and compression of the distal nose by displacing
the tension to the tissue reservoirs on the proximal and lateral nose and by keeping tension vectors parallel to the margins of the tip and ala (Fig. 39-17).18 They are especially useful when tension at the primary defect precludes primary closure or a sliding flap.
Three common transposition flaps are the rhombic (single-lobed), bilobed, and trilobed flaps (Fig. 39-17).18 The latter two flaps have a significant rotational component as well. Adding lobes to the flaps recruits tissue from reservoirs increasingly remote from the primary defect and displaces tension to more favorable vectors. Defects on the proximal nose and sidewall are immediately adjacent to the tissue reservoir, so the single lobe of the rhombic flap may be adequate (Fig. 39-18A).
Defects on the supra-tip and proximal nasal tip may require a bilobed flap (Fig. 39- 18B), and more distal defects may require a trilobed flap (Fig. 39-18C). In general, the angle between the defect, primary lobe, and secondary lobe dictates whether a trilobed flap is needed, as maintaining acute angles, ideally 45 degrees or less, results in tension-free flap motion.
As opposed to sliding flaps, which have the greatest tension at the primary defect, transposition flaps displace tension to the ultimate donor site (i.e., secondary defect of a
rhombic flap; tertiary defect of a bilobed flap; and quaternary defect of a trilobed flap). By transferring tension to the donor defects over the proximal and lateral nose, the transposition flap can be rotated to the primary defect under minimal tension.
Rhombic transposition flaps Rhombic flaps are useful to reconstruct smaller defects of the proximal nose and sidewall by recruiting tissue from the nasal root, sidewall, and cheek (Fig. 39-19). The flap extends from the midline of the defect toward the desired tissue reservoir. For nasal defects, the open limb of the flap usually points laterally (i.e., the flap has a laterally based pedicle), which eases closure of the donor site and helps to push the flap toward the defect. The classic rhombic flap has a 60-degree angle at its apex, but lengthening the flap to create a more acute apical angle can facilitate closure and avoid a standing cone deformity at the donor site.
To avoid secondary motion at the primary defect, the flap should have approximately
the same surface area as the defect and extend perpendicularly to the defect.18 The first key suture closes the secondary defect and bears the greatest amount of tension. The second key suture sets the flap into the primary defect and determines its arc of rotation as well as the position of the standing cone. As the arc of rotation increases, pivotal restraint effectively shortens the flap, making it more difficult for its distal edge to reach the defect, and the standing cone deformity may encroach on the flap pedicle. It is preferable to set the flap so that the standing cone deformity does not narrow the pedicle. Removing the standing cone is often reserved until the flap has been set in its ideal location.
The triangular shape of the distal flap does not correspond to typically circular defects. The surgeon can either trim the flap to match the defect or triangulate the defect to accommodate the flap. Since the distal flap has the most tenuous blood supply, it is usually preferable to trim the excess tissue of the flap to match the defect.
Bilobed flap If a rhombic flap is not possible because tension on the skin immediately adjacent to the primary defect is excessive or causes anatomic distortion, the bilobed flap can reach donor sites more remote from the defect. The flap is most useful for defects of the nasal tip and supra-tip (Fig. 39-18B). Compared to the rhombic flap, the geometry and execution of the bilobed flap are more complex.18–21
Like the rhombic flap, the bilobed flap also rotates approximately 90 degrees (Fig. 39-20). However, the bilobed flap distributes the rotation between the two lobes, each rotating 45 degrees. The second lobe adds a Z-plasty component that helps push the flap toward the primary defect. The tension vector to close the donor site for the secondary lobe (i.e., the tertiary defect) should generally be horizontally oriented (parallel to the alar rim) in order to prevent free margin displacement.
nasal tip. Note the nearly vertical orientation of the secondary lobe on the nasal dorsum. (B) Immediate postoperative appearance demonstrates preserved position of the free margins of the tip and alae. (C) The nose has good contour and an inconspicuous scar at long-term follow-up.
The first key suture closes the tertiary defect. On the nose, the first suture pushes the flap toward the primary defect more effectively when the final, open limb is positioned laterally (i.e., a laterally based bilobed flap) versus medially (i.e., medially based bilobed flap). The second key suture sets the primary lobe into the defect. The exact position of this suture may vary or require adjustment to create tension vectors that avoid anatomic distortion, to align the standing cone, and to adjust the sizing of the primary lobe. It is often preferable to ensure that closure of the standing cone deformity preserves contour, before trimming excess tissue for a precise fit. The secondary lobe will generally have excess length and require trimming to match the secondary defect.
Trilobed flap The trilobed flap has tissue mechanics similar to the bilobed flap with a few distinct advantages (Fig. 39-21). First, its third lobe allows the flap to reach tissue reservoirs increasingly remote from the primary defect, and it is particularly useful to reconstruct distal nasal defects. Second, the third lobe extends the arc of rotation to 120 to 150 degrees and may provide a more favorable tension vector to close the quaternary defect. Third, the additional lobe adds the benefit of another Z-plasty, which decreases the tension to transpose the flap, an important advantage when even mild tension at the distal nose can distort the free margins. Finally, the third lobe increases the width of the flap pedicle. If the orientation of the standing cone would cut into the pedicle of a bilobed flap, the increased pedicle size of a trilobed flap may improve blood supply.22
Nasolabial transposition flap The nasolabial transposition is a modified rhombic transposition useful to reconstruct
defects of the alar groove and ala (Fig. 39-22).23 The flap recruits tissue from the generous reservoir at the nasolabial fold. Since the alar groove and ala have scant fat, and since the skin is firmly adherent from the dermal insertions of the underlying muscles, this flap can appear too thick and pincushion without precise undermining plane and tacking sutures to recreate the alar groove.
The medial arm of the flap extends from the lateral aspect of the nasal defect down
along the nasolabial fold. The lateral arm of the defect extends along the cheek in a parallel line that gently tapers to join the nasolabial fold at its inferior aspect. The horizontal widths of the proximal flap and defect should be identical. The superior aspect of the cheek limb of the flap should remain a couple millimeters inferior to the origination point of the medial limb. This slight discrepancy is important to orient the primary tension vector in a superomedial vector that recruits skin from the mobile buccal cheek.
The flap is elevated to include only the subdermal fat. If it includes the nasolabial fat pad, the flap will have too much volume. The nasolabial fold and cheek are undermined in the same tissue plane.
The key suture closes the donor defect at the flap’s origination point. If the wound is under high tension, tacking the cheek to the origin of the transverse nasalis along the pyriform aperture may be necessary to avoid lateral distraction of the nose. The distal portion of the flap is trimmed to match the size of the defect, and it is sutured to the primary defect. The alar groove has a deep concavity, and the flap will pincushion if the dead space is not closed. Tacking the base of the flap to the caudal margin of the transverse nasalis muscle is usually necessary to close dead space and restore contour of the concave alar groove. Transposition of the flap creates a standing cone along the nasal sidewall, which is removed taking care to preserve the flap pedicle.
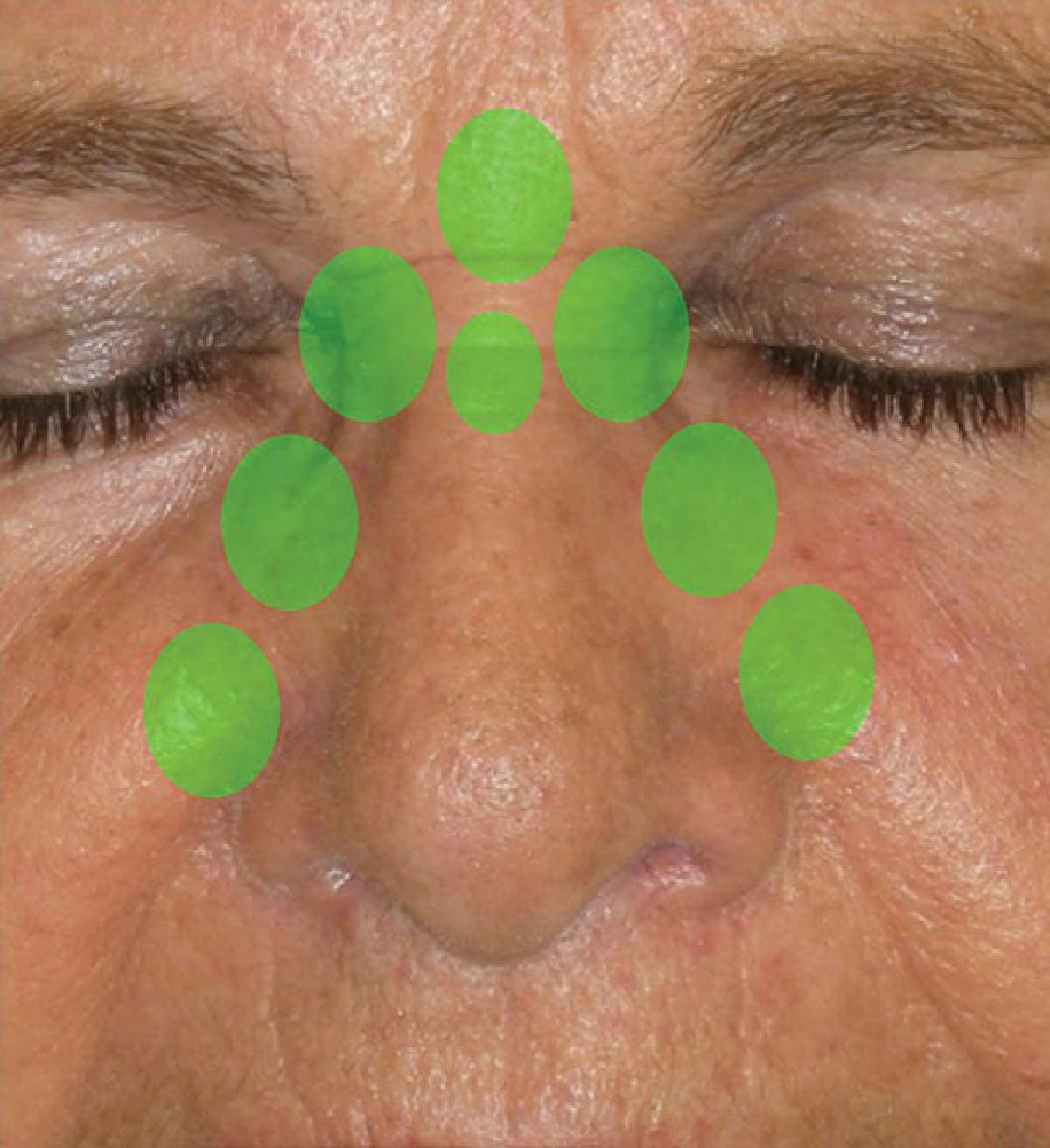
Figure 39-17. Tissue reservoirs on or near the nose. The green circles highlight tissue reservoirs for transposition flaps of nasal defects.
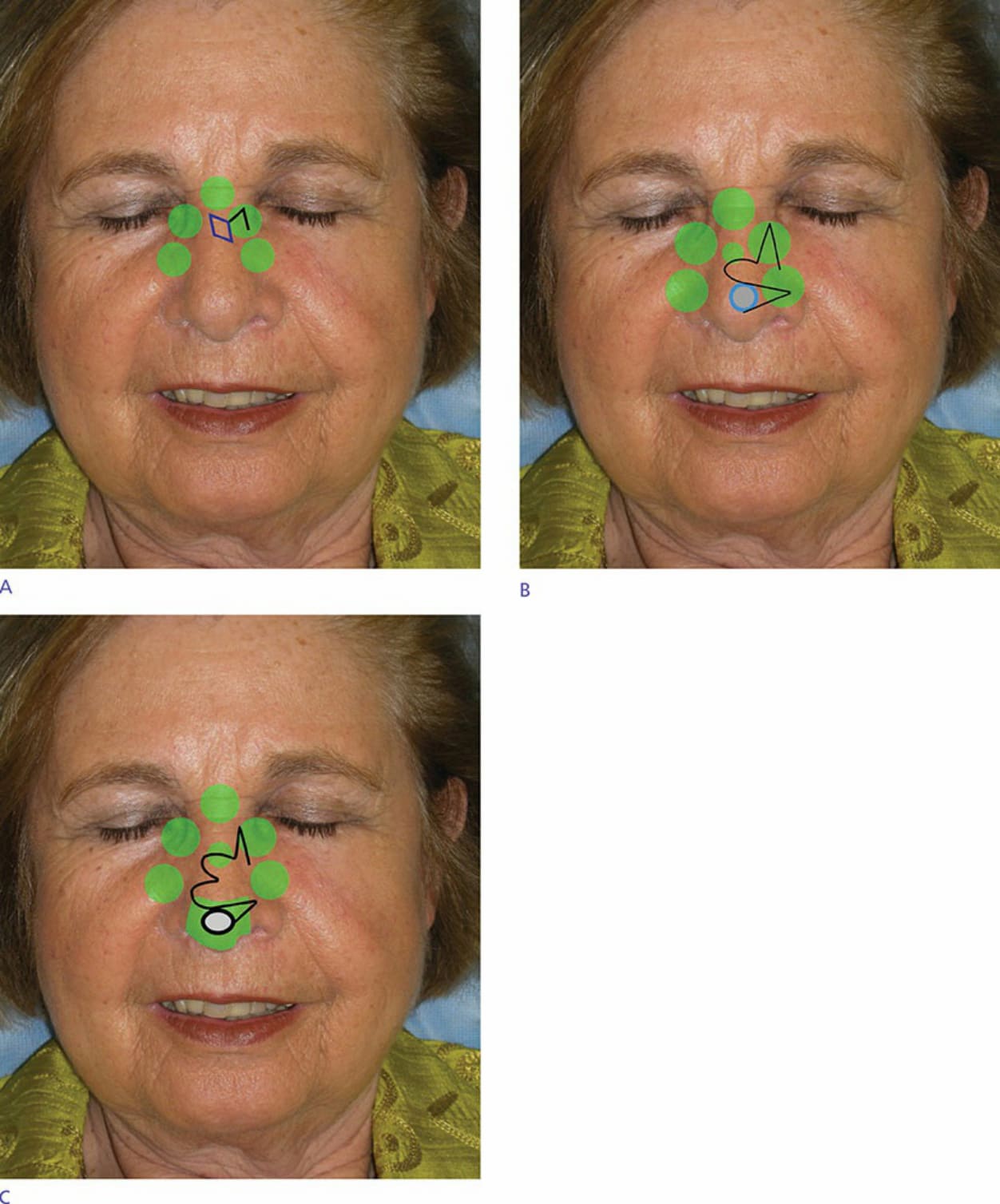
Figure 39-18. Transposition flaps for nasal reconstruction. (A) Rhombic flap. (B) Bilobed flap. (C) Trilobed flap.

Figure 39-19. Rhombic (single-lobed) transposition flap. (A) A rhombic flap is designed to recruit from the tissue reservoir immediately adjacent to this small defect. Note that the open limb of the flap points laterally. Tissue is recruited from lateral to medial, which pushes the flap toward the primary defect. (B) The flap has been transposed into the primary defect, and the standing cone has been excised along the alar groove. (C,D) At short-term follow-up, the scar is inconspicuous from the lateral and frontal views.

Figure 39-20. Bilobed flap. (A) A laterally based bilobed flap is designed to repair this moderately sized defect of the

Figure 39-21. Trilobed flap. (A) A laterally based trilobed flap is designed to repair a Mohs defect of the lateral nasal tip. The third lobe was necessary to ensure a horizontal (i.e., parallel to the alar rim) tension vector at the quaternary defect. (B) The position of the alar margin is preserved immediately postoperatively. (C,D) The nasal contour is preserved and the scar is inconspicuous at short-term follow-up.

Figure 39-22. Nasolabial transposition flap. (A,B) A nasolabial transposition flap is designed to repair a deep defect that spans the lateral alar groove. (C) Immediate postoperative appearance. The skin is tacked to the pyriform aperture to recreate the alar groove. (D,E) Contour is restored and the scar is minimally apparent at follow-up.