Rotation Flaps
Rotation Flaps
Rotation flaps distribute tension across multiple vectors to avoid the distortion that would occur from the single tension vector of an advancement flap. The hallmark of a rotation flap is the arciform incision used to mobilize the surrounding skin. Rotating the flap into the primary defect creates a secondary defect along the arciform incision. Tension is distributed with multiple vectors along both the primary and secondary defects. Three common nasal rotation flaps include the dorsal nasal rotation flap, the spiral flap, and the Peng flap.
Dorsal nasal rotation flap The dorsal nasal flap (DNF) is an axial rotation flap based on the DNA (Fig. 39-14).6,12
While the DNF may repair full-thickness defects13 and alar defects,14 it is most commonly used to reconstruct partial-thickness defects on the nasal tip or dorsum. The flap recruits skin from more lax areas of the proximal and lateral nose, allowing reconstruction of moderately sized distal defects without nasal distortion. Defects with a longer vertical axis are ideal for the DNF, since the flap’s redundant cone also occurs in this direction. Laterally based bilobed flaps may be better suited for distal midline and paramedian nasal defects with a longer horizontal axis.
appearance. Note the relative preservation of the shape of the nose. (D) The scar is minimally apparent.
The curvilinear arc of the flap takes off from the distal edge of the defect. Taking off from the proximal defect requires excessive advancement of the flap, which may lead to undue tension or nasal tip distortion. The arc sweeps from the distal defect across the lower nasal tip or cephalic border of the soft triangle and alar crease to the nasofacial sulcus, then continues cephalically to the medial canthus and transverse glabellar crease. A back-cut along the contralateral transverse glabellar crease may improve flap mobility, but it should preserve at least 7 mm of skin near the contralateral medial canthal tendon to protect the DNA. If the flap reaches the defect without tension, extension into the glabella is unnecessary.
The flap is elevated in a caudal to cephalic direction. The distal flap over the tip, sidewalls, and dorsum is elevated in the supraperichondrial plane deep to the nasalis muscle. At the root of the nose, the dissection shifts to a more superficial plane immediately above the procerus muscle. To improve the mobility of the flap, undermining extends toward the contralateral medial canthus, taking care to maintain the undermining plane just above the periosteum and preserve the DNA.
When the undermined flap slides toward the defect with minimal tension or nasal distortion, the redundant cone is removed. A vertically oriented standing cone decreases the size of the pedicle, but minimizes elevation of the tip and ala. A more horizontally oriented standing cone maximizes the size of the pedicle, but may result in the elevation of the tip or ala. Excising the standing cone to perichondrium will usually transect the lateral nasal artery. If the surgeon fears that the DNA may not supply sufficient blood to the distal flap, the lateral nasal artery may be preserved by excising the standing cone in the subdermal plane. However, the excess soft tissue may result in a bulkier contour.
The key suture for the DNF approximates the leading edge of the flap to the most distal or caudal portion of the defect. Minimal distortion of the nose should occur after placing this suture. The second key suture re-approximates the secondary defect along the nasofacial sulcus. Advancement of cheek skin is aided by undermining the cheek in the subcutaneous fat, immediately superficial to the levator labialis superioris alaeque nasi. Additional sutures are placed along the remainder of the flap, with careful attention to evert the skin edges, though hypereversion in the nasofacial sulcus should be avoided. If a glabellar incision is made, judicious thinning of the fat and dermis of the glabellar skin to approximate the thickness of the more delicate canthal skin may improve the contour match at the medial canthus. If a glabellar incision is not made, the surgeon may find that a small tissue redundancy may need to be removed by taking a Burow’s cone into the canthal area.
Spiral flap The spiral flap is a rotation flap with a tight arc between 180 and 270 degrees.15 The
flap is ideal for defects of the alar groove and lateral nasal tip (Fig. 39-15). Although the flap has a narrow pedicle and slim distal tip, the robust blood supply from the nearby lateral nasal artery keeps the flap viable.
The take-off point for the arciform incision is at the distal and medial aspects of the nasal defect. The arc extends in a three-quarter circle ending at the nasofacial sulcus. The flap is elevated with or without the transverse nasalis and rotated like a spiral toward the defect. The thin distal tip of the flap bends like a hook to recreate the alar groove. Partial necrosis of the thin distal tip may occur, but second-intention healing along the alar groove still results in a reasonable aesthetic outcome. The secondary defect along the nasal tip and sidewall is sutured with a layered closure.
Peng flap The Peng flap is a bilateral rotation flap used to repair defects of the nasal tip and distal dorsum (Fig. 39-15D).16 It can be conceptualized as a bilateral DNF. The take-off points of rotation flaps affect biomechanics: initiating the arciform incision from the distal defect makes the flap tips narrower and more vulnerable to necrosis, but the flaps require minimal distal advancement to reach the distal defect. Pivotal restraint shortens the flaps as they are rotated, so some upward secondary motion from the nasal tip is expected. Initiating the arciform excision from the proximal defect creates a broader flap tip, but the flap requires more distal advancement to cover the defect. Significant secondary motion may elevate the nasal tip.
Regardless of the take-off points, the flaps are rotated centrally and sutured at the midline nose. A standing cone forms at the superior aspect of the defect and requires excision to restore contour. A secondary defect forms along the lateral aspects of the arciform excisions. Closing the secondary defects may result in flaring of the ala or compression of the lateral crura of the lower lateral cartilages, especially if the flaps are used to repair distal nasal defects.
V–Y island pedicle flaps V–Y island pedicle advancement flaps differ from the other sliding flaps in that their entire blood supply comes from the flap’s undersurface (Fig. 39-16). A triangularshaped flap is designed with the base of the triangle at the edge of the nasal defect. Incisions are made through the dermis of the two remaining limbs, creating the “island” that gives the flap its name. The skin of the nose is relatively adherent to the underlying cartilage and muscles of facial expression, so the flap may not advance after releasing the dermis. In most cases, the underlying muscle must be incised on one of the flap limbs, and the flap is undermined deep to the muscle.17 The skin is released from the superficial aspect of the muscle on the opposite limb, and the flap usually gains enough mobility to advance toward the defect. If the flap is still restrained, the muscle pedicle may need to be partially incised. While incising the muscle on both sides of the flap may increase the mobility, it may threaten the viability of the flap.
Once the flap is sufficiently mobilized, a key suture advances the leading edge of the flap toward the defect. Secondary motion is expected, particularly if the flap is still restrained. The secondary defect at the trailing edge of the flap is closed primarily, resulting in a suture line that resembles a “Y.”
To avoid elevation of the tip and ala, the flap is usually designed to recruit skin along a horizontal vector from the nasal sidewall or lateral ala toward the midline. V–Y flaps may also be designed to move from superior to inferior, though elevation of the tip and ala is then more likely.

Figure 39-14. Dorsal nasal rotation flap. (A) A dorsal nasal flap is designed to repair this tall, distal nasal defect. (B) Intraoperative photo demonstrating the planes of dissection. The dorsum and tip are elevated superior to the perichondrium. The root and glabella are dissected in the supramuscular plane. (C) Immediate postoperative
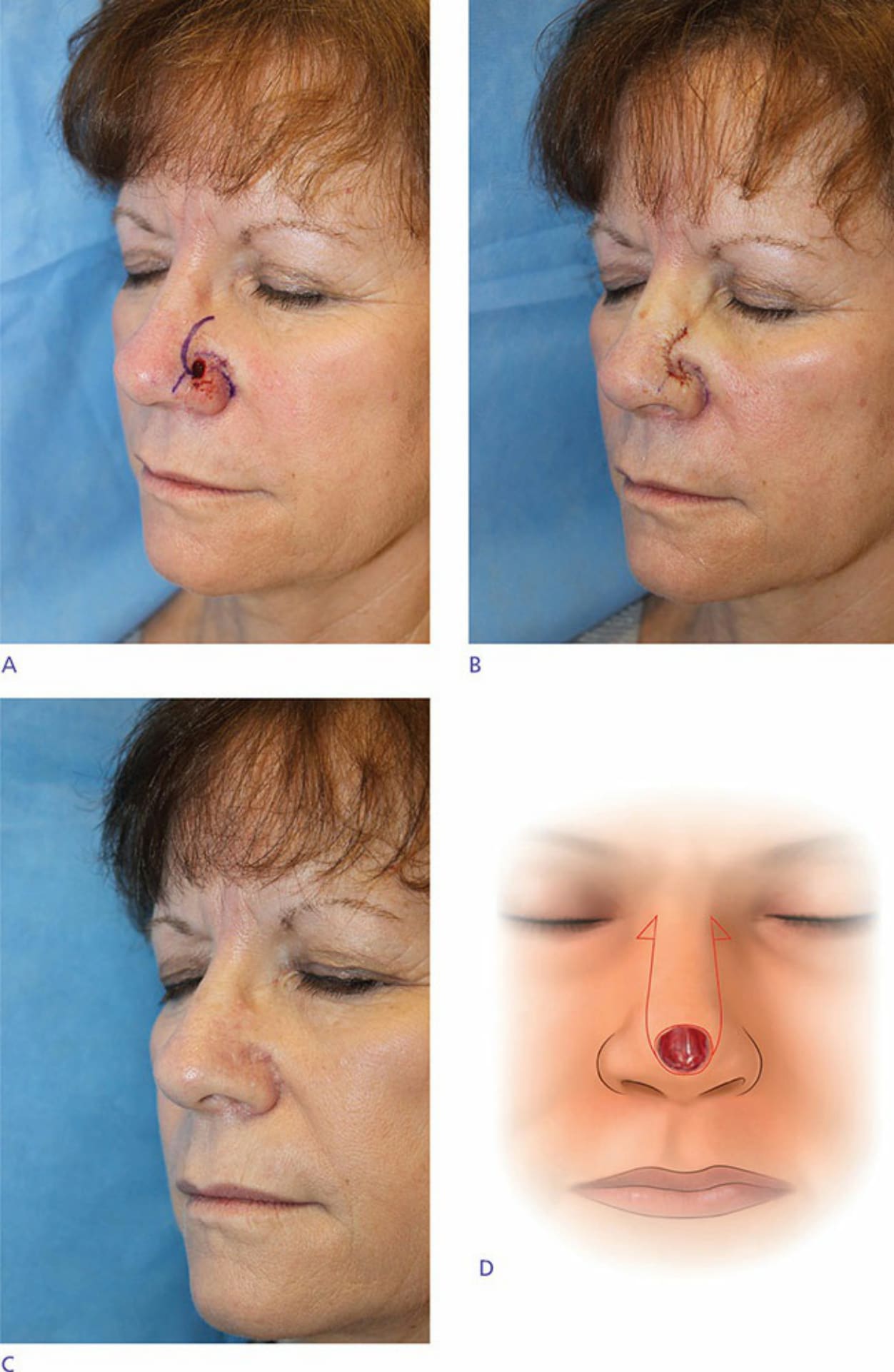
Figure 39-15. (A) A spiral flap is designed to repair this small, deep defect of the anterior alar groove. (B) Immediate postoperative appearance. (C) Inconspicuous scar with longer-term follow-up. (D) The Peng flap is a bilateral rotation flap used to repair defects of the nasal tip and distal dorsum.

Figure 39-16. Example of V–Y island pedicle advancement flap. (A) A small, deep defect on the anterior alar groove. (B) The wound is extended in a column to the alar margin, and a V–Y advancement flap is incised in the alar groove and free margin. (C) The flap is advanced anteriorly on its pedicle, leaving a secondary defect along the posterior alar groove. (D) Appearance immediately after surgery. (E) Postoperative appearance with inconspicuous scar and preserved nasal contour.