Advancement Flaps
Advancement Flaps
Advancement flaps have a random-pattern blood supply and are useful for wounds that could be closed with a fusiform excision, except one of the standing cones falls in an unfavorable position. As noted in the section on primary closure, fusiform excisions on the nose usually require a vertical orientation to prevent lifting the free margins. The
superior standing cone can usually be excised freely, but the inferior standing cone may encroach upon the margin of the ala and tip. In these instances, an advancement flap maintains tension along the same single vector as the primary closure but displaces the inferior standing cone to a more favorable position at the cheek or columella.
For wounds of the lateral nose, an advancement flap (Burow’s flap) may shift the inferior standing cone away from the ala to the nasolabial fold. This unilateral advancement flap is ideal for wounds located entirely superior to the alar groove, because the lateral scar may be completely disguised in the nasolabial fold, and the skin can be advanced with a superomedial vector (Fig. 39-12). If the wound involves the alar groove, a transposition flap is usually preferable, because attempting to advance the cheek skin inferomedially usually lifts the ala. For wounds of the paramidline, an advancement flap may extend the scar medially and shift the inferior standing cone away from the soft triangle to the columella (Fig. 39-13).11
This unilateral advancement flap is limited to small wounds, because excising too much skin from the narrow columella can give the nose a pinched appearance.
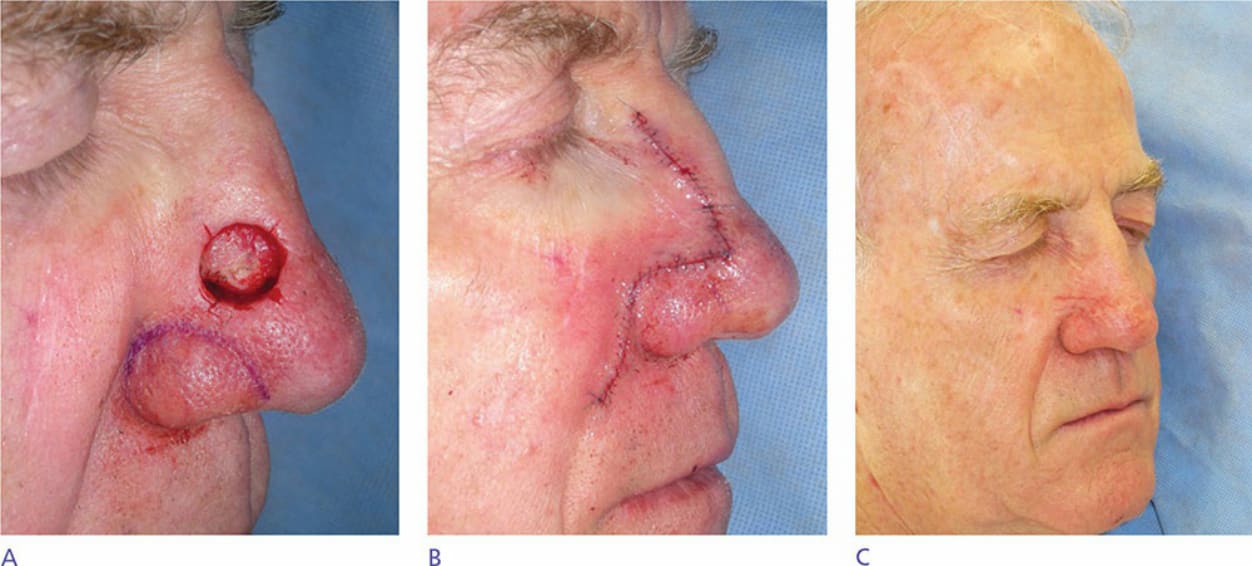
Figure 39-12. Unilateral advancements flaps are useful to repair defects of the nasal sidewall. (A) Mohs defect of the right nasal sidewall. A vertically oriented fusiform repair would encroach on the alar rim. (B) Immediate postoperative appearance of a unilateral advancement flap. The flap is designed to disguise the horizontal incision in the alar groove, and the inferior standing cone is displaced to the nasolabial fold. (C) Aside from the telangiectasias, the scar is minimally apparent.

Figure 39-13. (A) An “east–west” advancement flap is designed to displace the inferior standing cone to the midline nose during the repair of this tall, paramedian defect. (B) Appearance immediately postoperatively. The wound tension causes temporary alar flare, but the nasal bone and septal cartilage resist compression. (C) Postoperative appearance at 1 week. (D) Longer-term follow-up.