Ectropion Repair
Ectropion Repair
Simple cicatricial ectropion in the absence of pre-existing lid malposition can be corrected with a flap or graft that lengthens the anterior lamella combined with canthal suspension (Fig. 38-22).45–49 Early intervention is best, before wound contraction is
severe. Repair begins with excising the scar and estimating the size of the defect on maximal stretch of the lower lid with upward traction. The defect size can be estimated by blotting the area with a sterile nonadherent gauze pad. The flap or graft can then be appropriately designed to provide ample coverage on maximal stretch. Pushing flaps, such as inferiorly based rhombic transposition flaps or superiorly based Tripier-type transposition flaps combined with a lateral canthopexy, are often straightforward and satisfactory.47,48 Full-thickness skin grafts sized adequately with the lid on full stretch, tacked down, and combined with a canthopexy suture or a full lateral tarsal strip are reliable for even some of the most severe ectropion.49 A modified Frost suture is generally beneficial to counteract the downward traction and is left in place for 7 to 10 days.
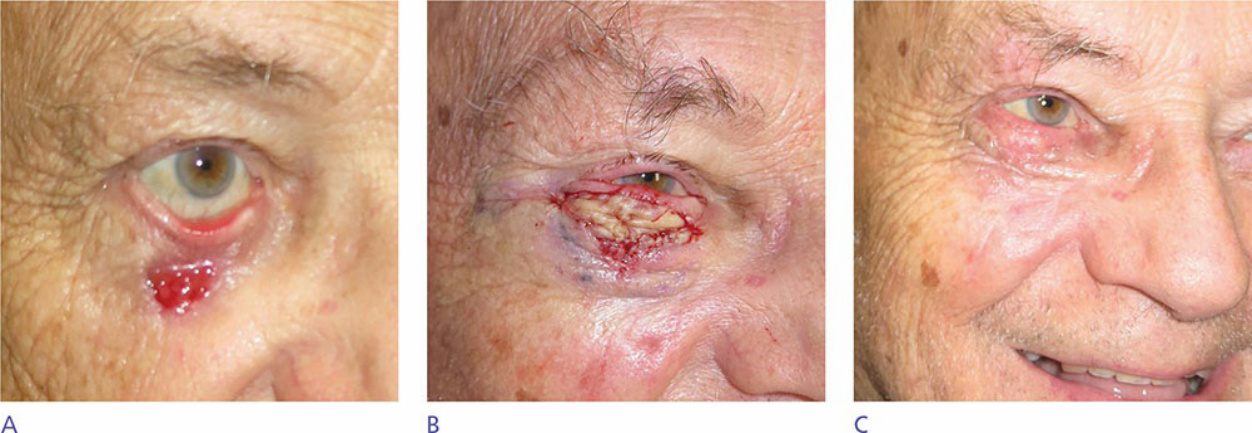
Figure 38-22. Ectropion repair. (A) Low-lid ectropion 3 weeks after the repair was delayed following Mohs surgery. (B) Oversized full-thickness skin graft designed with lid on maximal stretch. (C) Ectropion repaired 2 weeks postoperatively.