MEDIAL CANTHUS
MEDIAL CANTHUS
The complex anatomy of the medial canthus creates distinct challenges for the periocular surgeon.29,30 Though it may worsen with age, the propensity of medial canthal skin to form a web is fairly constant. Webbing across the canthus occurs readily if not actively prevented, due to its concave contour, the need for vertical movement of the brows, and the thin mobile skin inside the orbital rim adjacent to the relatively thicker bound skin of the cheek and nose. Fundamental principles of reconstruction in the medial canthus that minimize risks of webbing include designing flaps within the canthal subunits, sizing flaps, and grafts adequately to cover the concavity of the canthi
and accommodate vertical movement of the muscles of facial expression, and suspending flaps to the periosteum and canthal support tissues to direct tension.12–14 Conceptually, the subunits of the medial canthi are defined by the attachments of the orbital rim that separate the more thin mobile skin inside the orbit from the thicker bound skin of the cheek and nose, and the horizontal apex of the medial canthus (Fig. 38- 13).14 Combining flaps within the canthal subunits and suspending them to the canthal support tissue is a cornerstone of repairing canthal defects to reliably avoid webbing.12
Owing to its innate concavity and complex anatomy, second-intention healing and skin grafting are often used for defects in the medial canthus.31–33 Second-intention healing is ideal for small, superficial defects near the apex of the canthus. Full-thickness skin grafts are also commonly used to repair medial canthal defects, and even for deeper defects particularly when tumor surveillance is a high priority.
Nevertheless, flap repairs in the medial canthus often optimize outcomes and help avoid the drawbacks and limitations of grafts and second-intention healing. For defects located at or superior to the canthal apex, hatchet-type rotation flaps based on the glabellar skin are ideal (Fig. 38-14).34 Incisions can be obscured in natural rhytids, and the tissue reservoir is ample, so flaps rotate freely into the canthus. The flap base can provide bulk for deeper defects or can be thinned for superficial defects, and can be easily suspended to the canthal tendon to preserve the natural canthal concavity. The high degree of mobility and minimal visible scarring make this flap a workhorse in this area. Glabellar rotation flaps can be combined with a number of inferiorly based flaps to repair larger defects that include the superior aspect of the medial canthus.35 The canaliculi can be probed and canalized with care not to traumatize them to ensure patency when indicated.28 Damage to the lacrimal drainage system may require reconstructing; however, many patients, particularly elderly patients with dry eyes, benefit from the disruption and do not require repair.
Island pedicle (V–Y type) advancement flaps suspended to the periosteum or canthal tendon can be ideal for superficial and deep defects located at or below the canthal apex, including deeper defects that breach the orbital septum (Fig. 38-15).36–41 Incision lines can be partially obscured in the shadow of the nasofacial sulcus, and the medial cheek skin moves readily above the malar fat pad. Island pedicle flaps can be suspended to the periosteum or canthal tendon to preserve the contour of the canthus. Island pedicle flaps are advantageous in this area because they have immense mobility with minimal undermining, do not require removal of redundant cones, and are easily and efficiently designed and executed. These flaps are best designed with adequate
length to avoid webbing, yet slightly undersized width to avoid pin-cushioning. Like blepharoplasty surgery, when the orbital septum is breached, the flap is mobilized and suspended into place without suturing the orbital septum. The septum is left to heal naturally to avoid tethering and lid retraction with wound contraction.
Larger defects can be repaired with a combination of rotation, transposition, or advancement flaps to avoid webbing. Bilateral rhomboid transposition flaps that direct redundant cones toward the canthus to avoid webbing are useful for larger medial canthal defects (Fig. 38-16). The largest medial canthal defects may require full-
thickness skin grafts from remote sites or two-stage interpolation flaps from the forehead to provide adequate tissue coverage.
For smaller defects close to the lid margins, lid advancement flaps based on lax lid skin are ideal (Fig. 38-17). Incisions are made close to the lash line and advanced horizontally to minimize risk of webbing. Suspension sutures can be useful to support flaps during wound contraction, even for the smallest of defects.
Suspension sutures can be placed in the periosteum or the medial canthal tendon.12–14 An intimate knowledge of the vascular anatomy of the medial canthus and a welldeveloped tactile sensitivity are essential for precise placement. Suspension sutures are placed through the medial canthus by advancing the needle through the periosteum or canthal tendon, entering and exiting at a shallow angle, and avoiding excessively deep penetration through the underlying lacrimal sac. Flaps are secured at the concavity within the canthus.
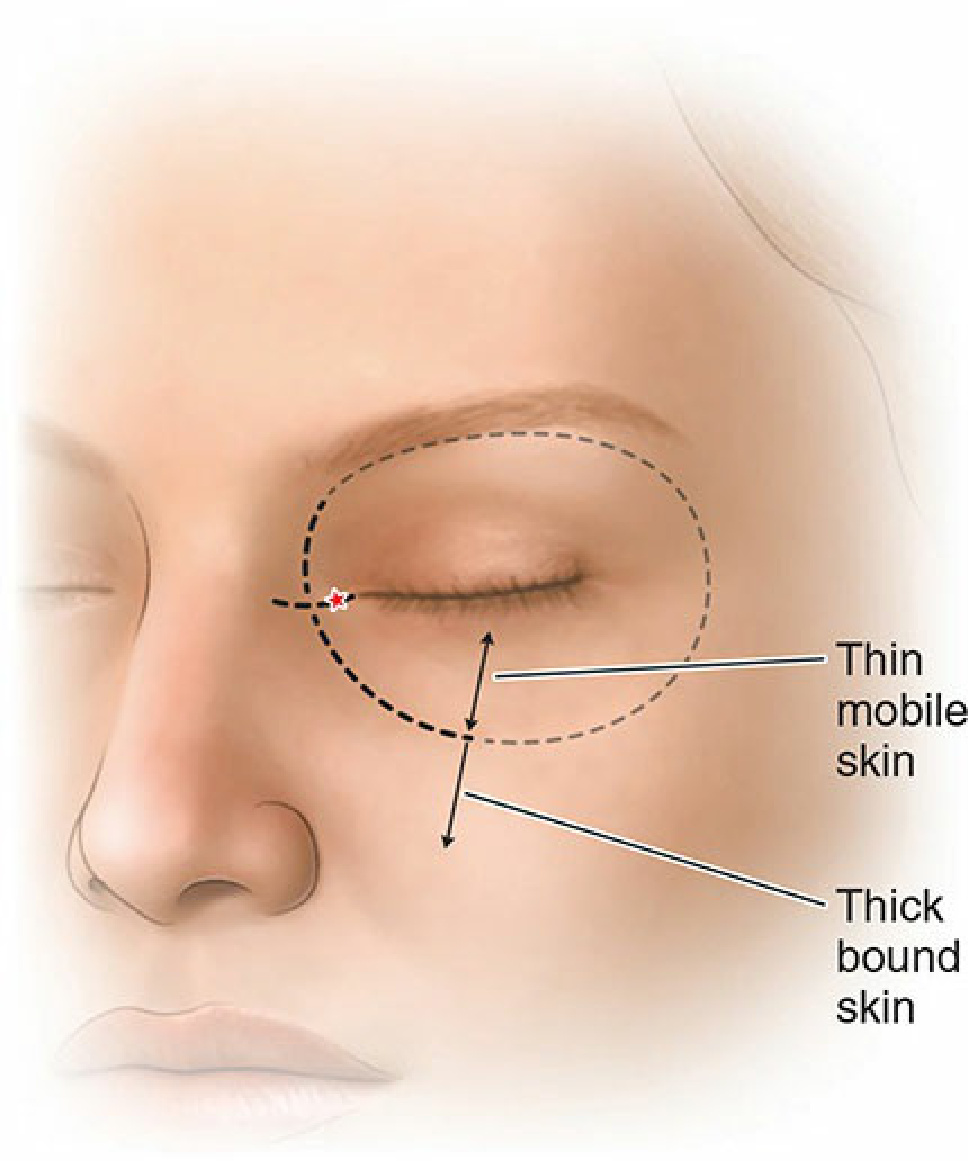
Figure 38-13. Medial canthal subunits: Combining flaps within the canthal subunits and suspending them to the canthal support tissue (*) is a cornerstone of repairing canthal defects to reliably avoid webbing. Skin inside the orbital rim is thin and mobile compared to thicker bound surrounding skin, easily contracting with tension.
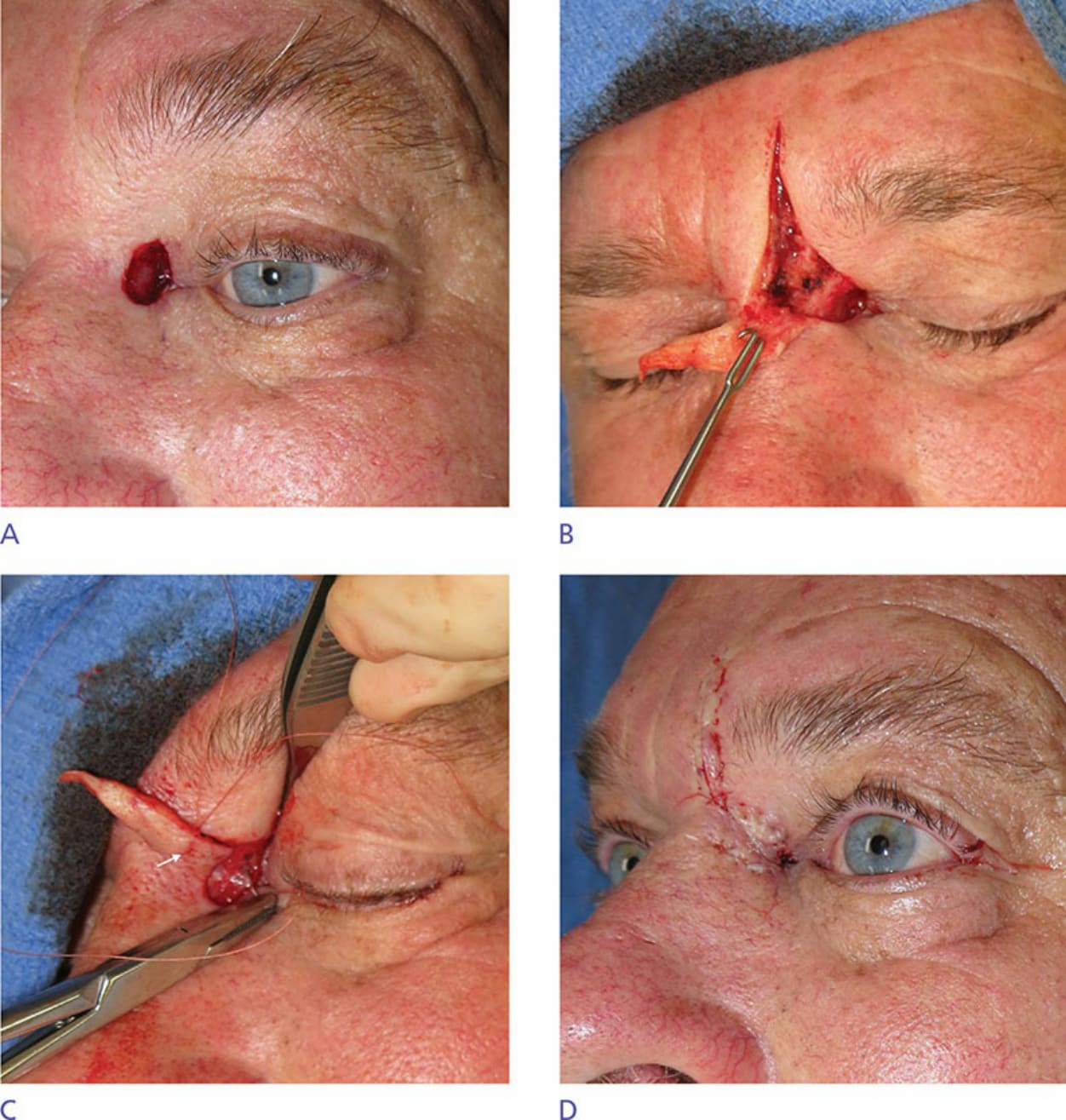
Figure 38-14. Hatchet flap. (A) Medial canthal defect at and above the canthal apex. (B) Flap based on the ample glabellar reservoir undermined in the mid fat with incisions placed in preexisting rhytid. (C) Suspension suture placed in the medial canthal tendon and 1 cm from the flap edge. (D) Canthal concavity preserved with maximal tension postoperatively.

Figure 38-15. IPF with canthal suspension. (A) Medial canthal defect at and below the canthal apex (arrow indicates medial canthal tendon and orbital fat pad). (B) Flap based on the mobile malar fat pad with suspension suture placed in the medial canthal tendon and 1 cm from the flap edge. The orbital septum is left to heal without suturing to prevent tethering. (C) Tension-free flap with concavity preserved and punctum in the lacrimal lake 2 weeks postoperatively.

Figure 38-16. Double rhomboid flaps. (A) Large defect involving the canthus to the nasal root. (B) Two rhomboid transposition flaps are designed above and below the defects. (C) Well-healed flap without webbing 5 years postoperatively.
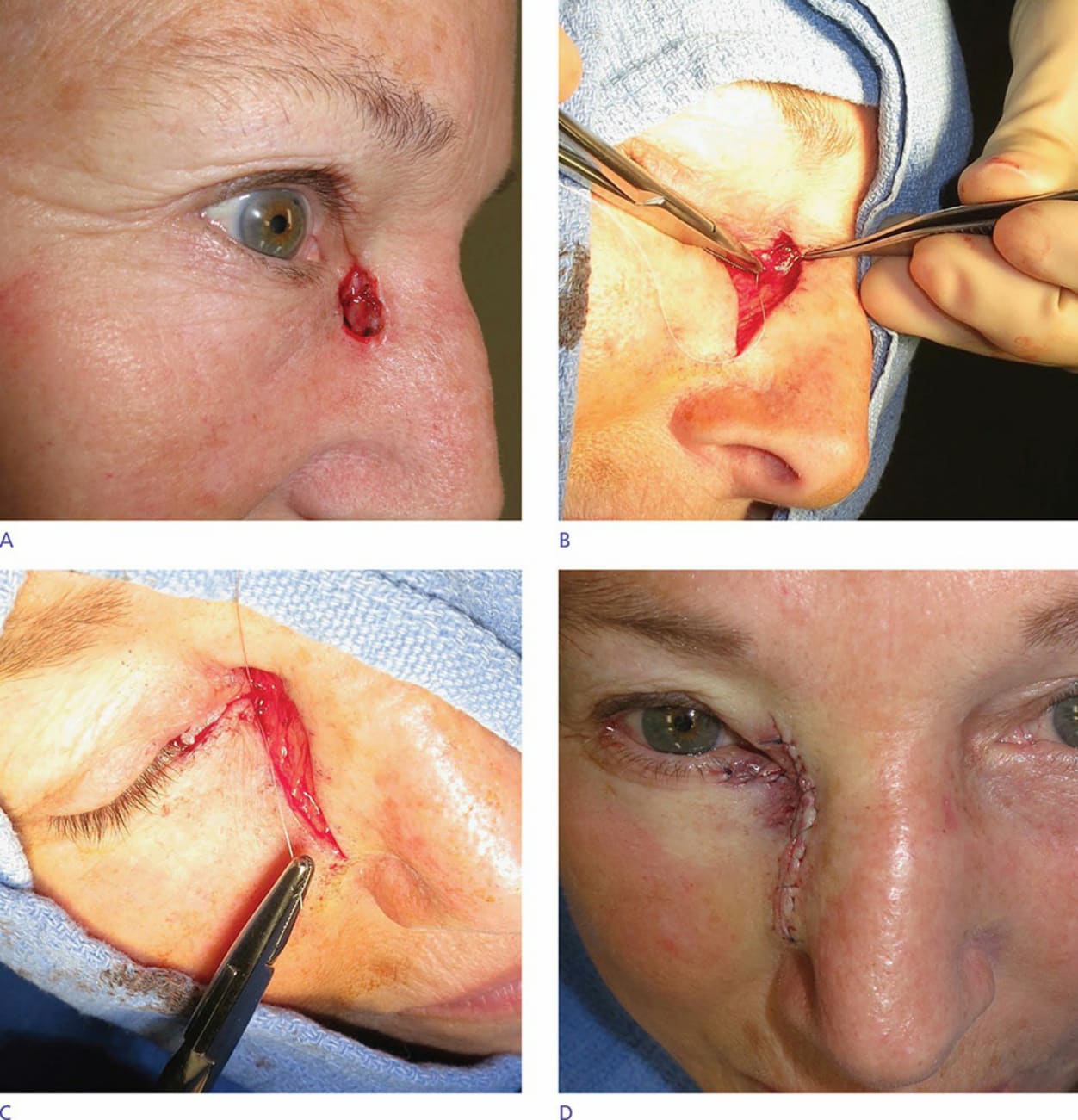
Figure 38-17. Lid advancement flap. (A) Vertically oriented defect below the medial canthal apex. (B) A subciliary incision is made, flap undermined, and suspension suture placed in the medial canthal tendon. (C) Canthal suspension suture is gently tightened with graduated tension. (D) Concavity is preserved with no vertical tension postoperatively.