UPPER LID
UPPER LID
Defects involving the skin and muscle of the upper eyelid are routinely repaired with flaps and grafts fashioned from the adjacent or contralateral eyelid (Fig. 38-11). Flaps and grafts such as these provide tissue and robust vascularity for rapid wound healing and can often be hidden in natural creases. Blepharoplasty-type advancement flaps based on the lid crease can be ideal for superficial defects on the upper lid where the incision lines are made along the natural lid crease and redundant skin and muscle of the crease can be easily mobilized into defects (Fig. 38-12). Just as in a simple blepharoplasty, incisions are kept lateral to the caruncle and may extend beyond the lateral canthus when hooding is present. Full-thickness defects of the upper lid often require the expertise and management of an oculoplastic surgeon to preserve the functional components of the upper lid.
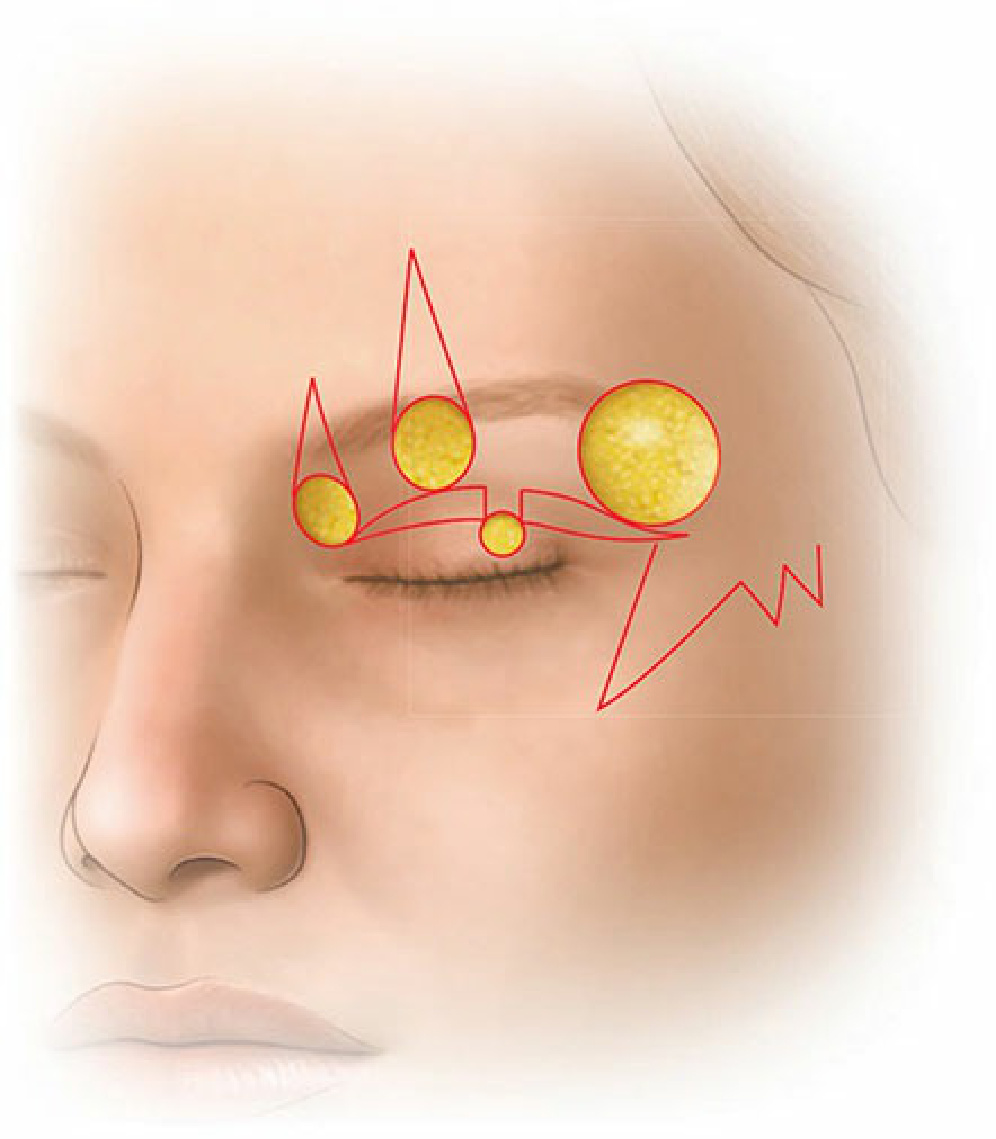
Figure 38-11. Defects on the upper lid can often be repaired with traditional or blepharoplasty-type advancement flaps with incisions along the lid crease. Transposition flaps can be useful for large defects.
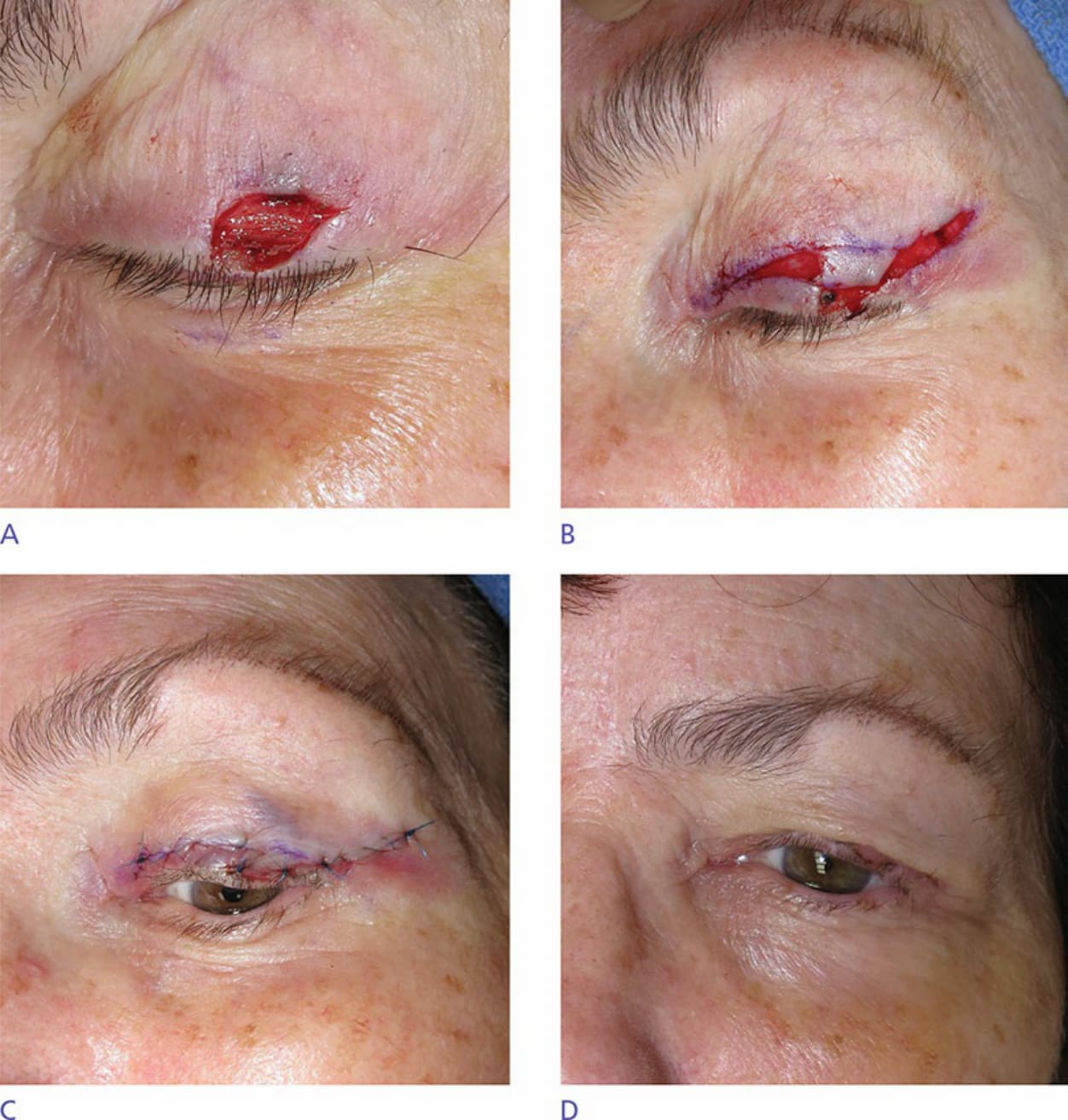
Figure 38-12. Blepharoplasty advancement flap. (A) Defect on the upper lid extending to the margin. (B) Flap incised with redundant cones removed from the upper lid crease. (C) Flap in place postoperatively. No sutures are placed along the lid margin to avoid irritation and corneal abrasion. (D) Tension-free flap 1 week postoperatively.