Flaps
Flaps
Numerous flaps have been used to successfully reconstruct the periocular area.19,20 While the characteristics of the defect and the surrounding tissue will determine the appropriate repair, a regional approach to periocular repairs according to surgical zones can be useful (Figs. 38-3 and 38-4).13,21–23 Regardless of choice of repair, it is imperative to design and support flaps and grafts in the perioperative period to minimize forces of gravity, edema, and wound contraction that may distract the lid away from the globe, causing complications of lid malposition, corneal exposure, lacrimal dysfunction, or suboptimal cosmesis. Ancillary suspension sutures, including medial and lateral canthopexy procedures, are used routinely during periocular repairs to prevent ectropion, especially in elderly patients with significant laxity, even if the eyelid or canthal support system is not disrupted by tumor extirpation.21,13 The following is a regional approach to periocular reconstruction and canthal support procedures that reliably repairs anterior lamellar and full-thickness lid defects.
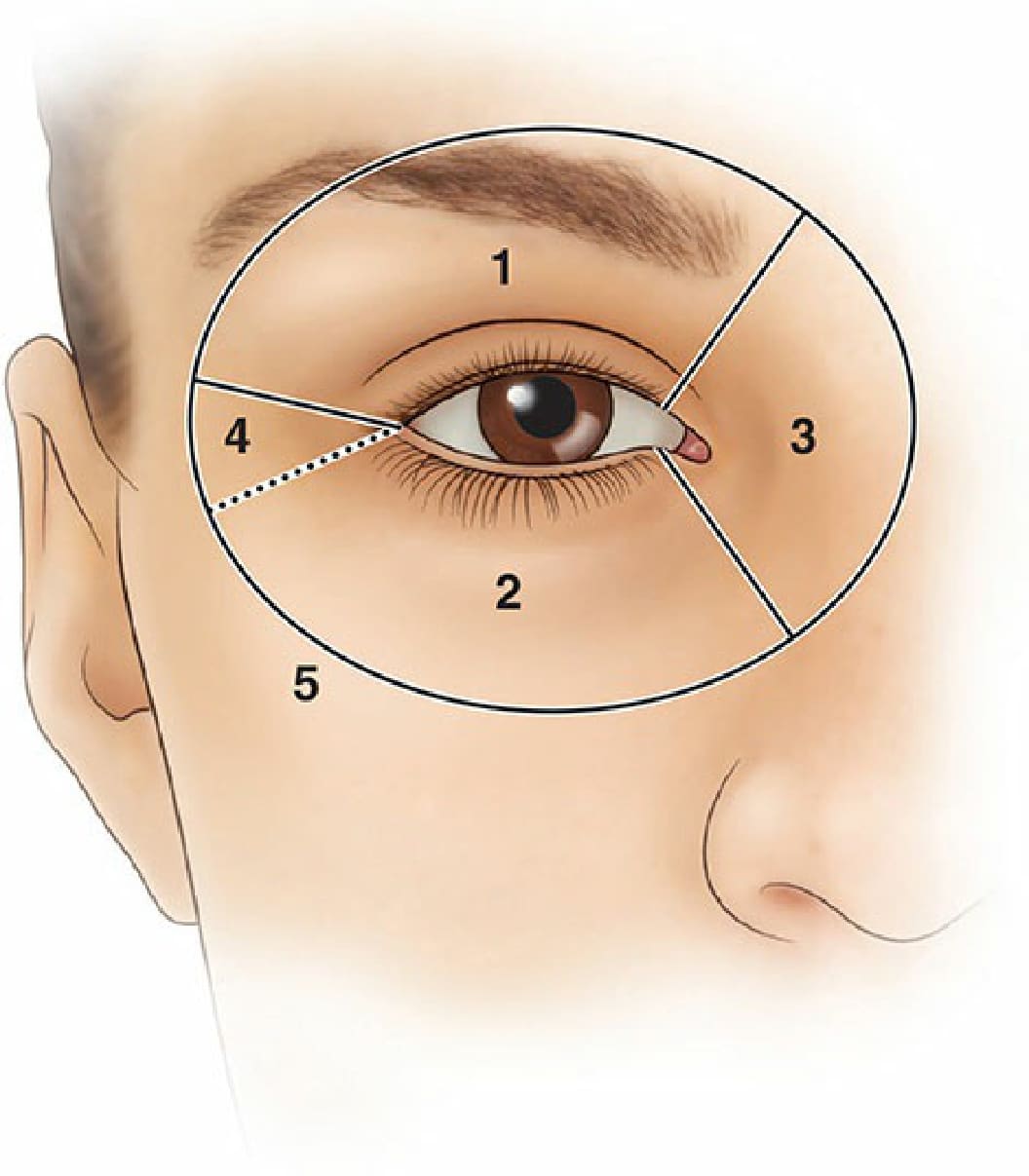
Figure 38-3. Modified zones of periocular reconstruction. Reconstructive options in the periocular region can be classified by surgical zone. 1. Upper lid. 2. Lower lid. 3. Medial canthus. 4. Lateral canthus. 5. Periorbital cheek. Reconstructive options for zones 2 and 4 are similar.
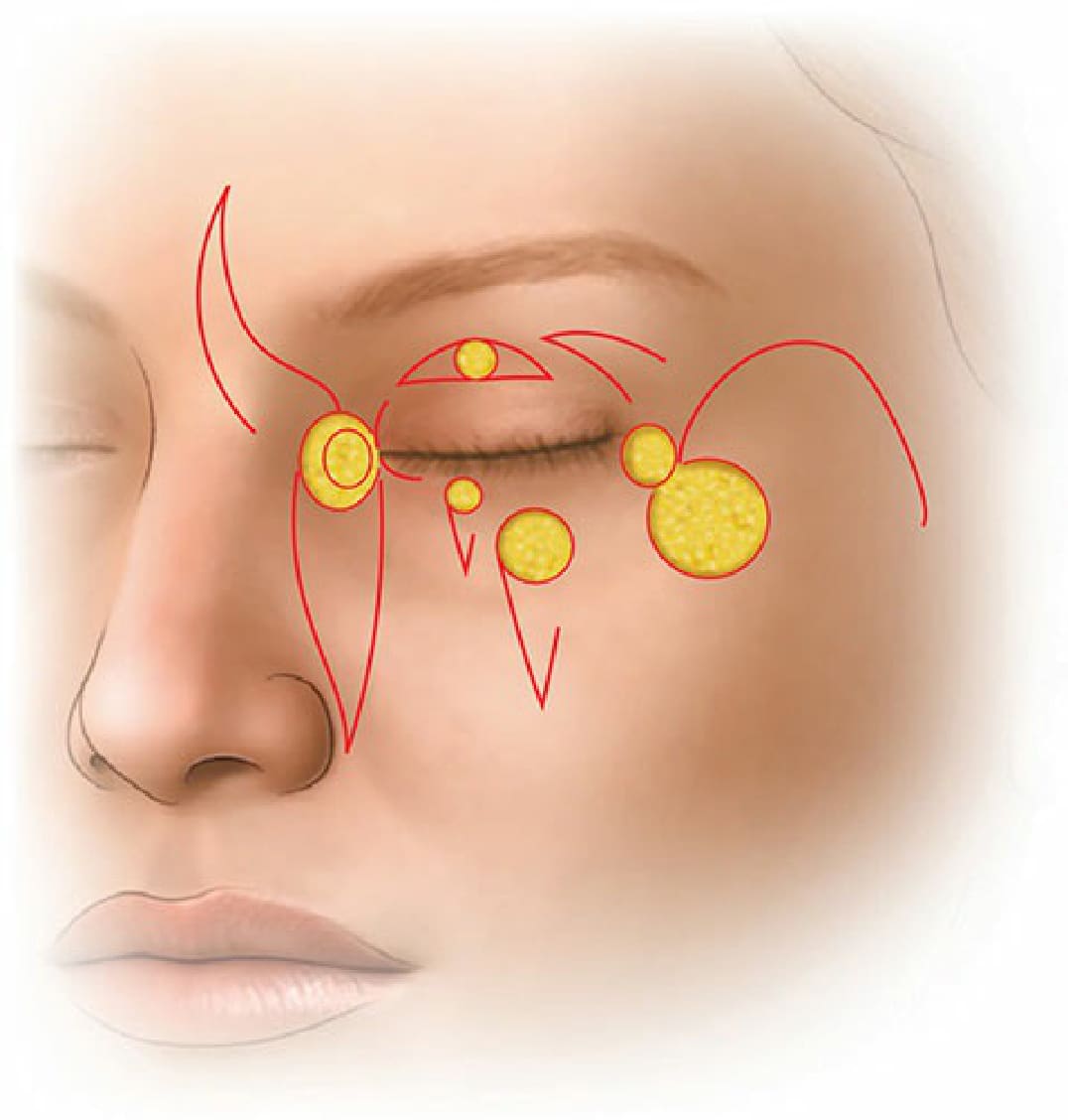
Figure 38-4. Regional approach to periocular flap repairs.