Linear Repairs
Linear Repairs
Linear repairs of wounds around the eye require a balance of keeping incisions perpendicular to the lid margin and obscuring incisions in relaxed skin tension lines (RSTL). Vertical incisions below the lid margin can be made in an increasingly oblique manner around the lower eyelid, except in the medial canthus where horizontal incisions are strictly avoided to prevent webbing (Fig. 38-2). Deep sutures can help to guide tension horizontally to allow for more oblique skin incisions. M-plasty repairs or simply leaving redundant cones can be useful for defects close to the lid margin. Small defects located on the upper lid crease can often be repaired with a traditional crescentshaped blepharoplasty incision along the natural crease, keeping incisions lateral to the caruncle to avoid webbing and extending beyond the lateral canthus when hooding is present. Due to the mobility of skin inside the bony orbit relative to the surrounding thicker bound periorbital skin, even defects outside the orbit that are repaired with incisions directed perpendicular to the lid margin can result in ectropion during wound contraction if the lid is sufficiently lax. Evaluating tension on the lid intraoperatively can help identify excessive tension. Periosteal suspension sutures can be placed around the eye when needed to support the lid during the perioperative period.7–11
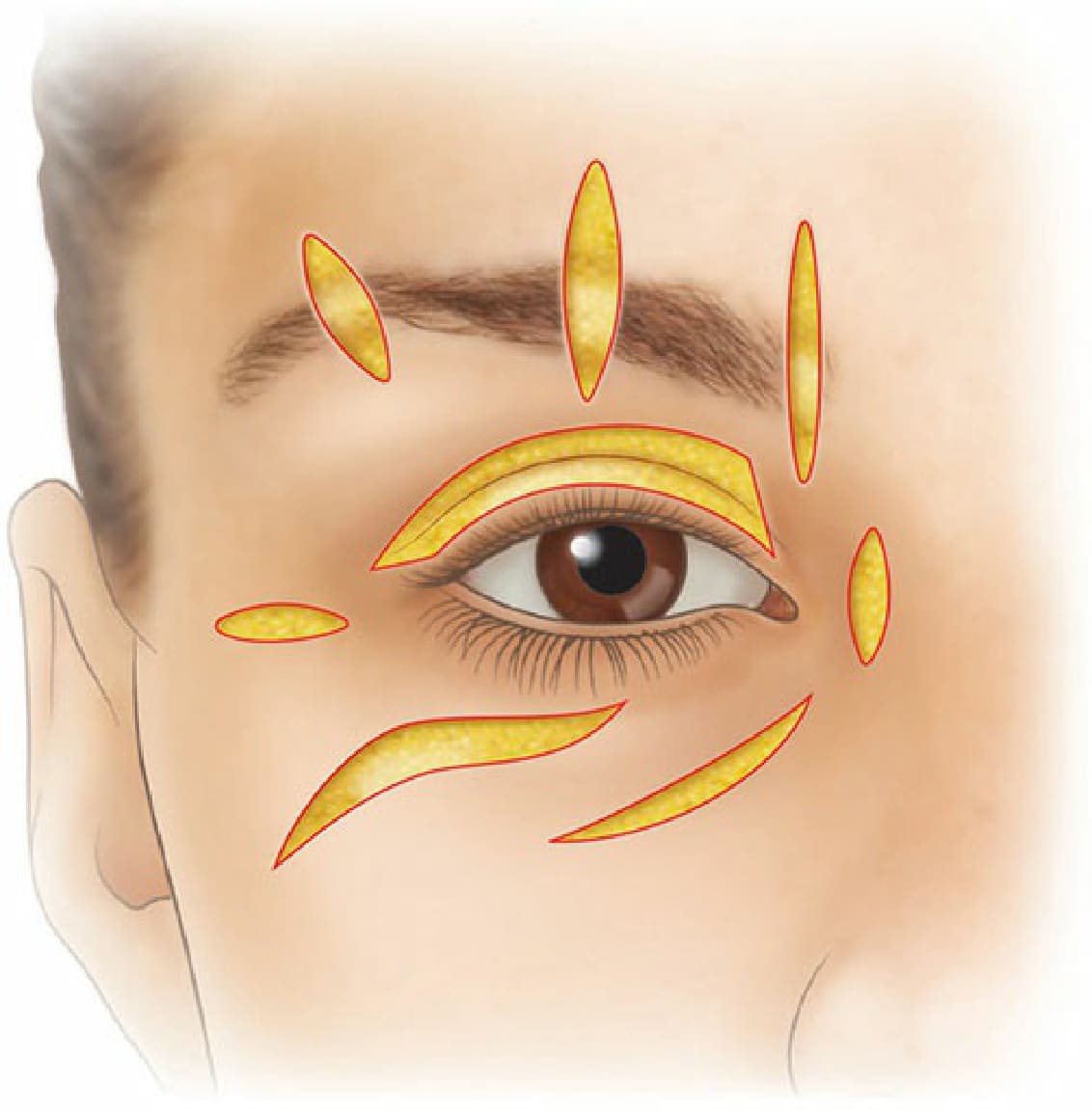
Figure 38-2. Linear repairs balance incision lines perpendicular to the lid margin and within relaxed skin tension lines. Vertical incisions can be made in an increasingly oblique manner around the lower lid, except in the medial canthus where horizontal incisions are strictly avoided to prevent webbing. Incisions on the upper lid can be made within the natural lid crease.