ANATOMY
ANATOMY
A comprehensive understanding of the distinct anatomic features of the eyelids is necessary for repairing surgical defects of the eyelids and periocular skin.3 The eyelids are a multilaminar structure comprising conjunctiva, tarsus, muscle, and skin, with various incorporated glands and appendages. The eyelids are suspended firmly to the bony orbit by tendons at the lateral and medial canthi and loosely surrounding soft tissue layers. Eyelids protect the globe and harbor glands that create the outer oil layer of the tear film required for clear vision. The relationships and attachments between the eyelid and surrounding soft tissue are essential for eyelid mobility and are the crux of expression and beauty.
The upper lid tarsus is curved in the shape of the globe where it rests smoothly along the surface with the medial puncti exposed to the lacrimal lake on blinking. The skin of the eyelid is thin, adherent over the tarsus of the palpebral lid. The posterior edge of the lid margin is sharper than the more rounded anterior edge with emanating lashes. This anatomic feature is a useful landmark for primary lid closures. The tarsus provides the structural support of the lid. The tarsus also houses the meibomian glands, which secrete the oily portion of the tear film that keeps tears from evaporating.
Conceptually, the lid is divided into anterior and posterior lamella, defining a plane of surgical division, which may be reconstructed independently. The posterior lamella is comprised of the conjunctiva and tarsus, the structure of the lid, and its mucosal lining, while the anterior lamella is comprised of the skin and orbicularis muscle. The orbicularis muscle consists of the orbital portion, which acts like a sphincter by forming an ellipse within the orbit and converging at the medial raphe of the canthus, and the tarsal and septal palpebral portions, which overly the upper and lower tarsi, respectively.
The palpebral orbicularis oculi muscles become contiguous with canthal tendons laterally before attaching to Whitnall’s tubercle, a bony prominence inside of the bony orbit, 4 mm posterior to the orbital rim just superior to the canthal apex. Whitnall’s tubercle is also the site of convergence of Whitnall’s and Lockwood’s ligaments, the pulley system of the lid motion and the supportive tissues of the lateral retinaculum. Medially the orbicularis muscle forms the complex structure of the lacrimal pump,
dividing into superficial and deep heads around the lacrimal canaliculi before attaching to the bony orbit at the maxilla and anterior and posterior lacrimal crests housing the lacrimal sac.
The vascular supply of the upper and lower eyelids supplied by the internal and external carotid arteries is comprehensive and generous, allowing for ready healing of surgical wounds (Fig. 38-1). Inferiorly the facial artery joins the dorsal nasal artery at the medial canthus just medial to the attachment of the canthal tendon to supply the upper and lower lids. The superficial temporal, lacrimal, and transverse facial arteries anastomose to form upper and lower palpebral arcades.
The muscular innervation of the orbicularis is supplied by numerous branches of the facial nerve, which are responsible for both the constitutive tone as well as the active sphincter-like motion of the orbicularis. When muscular innervation is compromised, osteocutaneous suspension sutures are useful to maintain the position of the eye and prevent ectropion. Sensory innervation of the orbicularis is supplied by numerous branches of the trigeminal nerve. Sensory and sympathetic motor nerves of the globe originate from the ciliary ganglion.
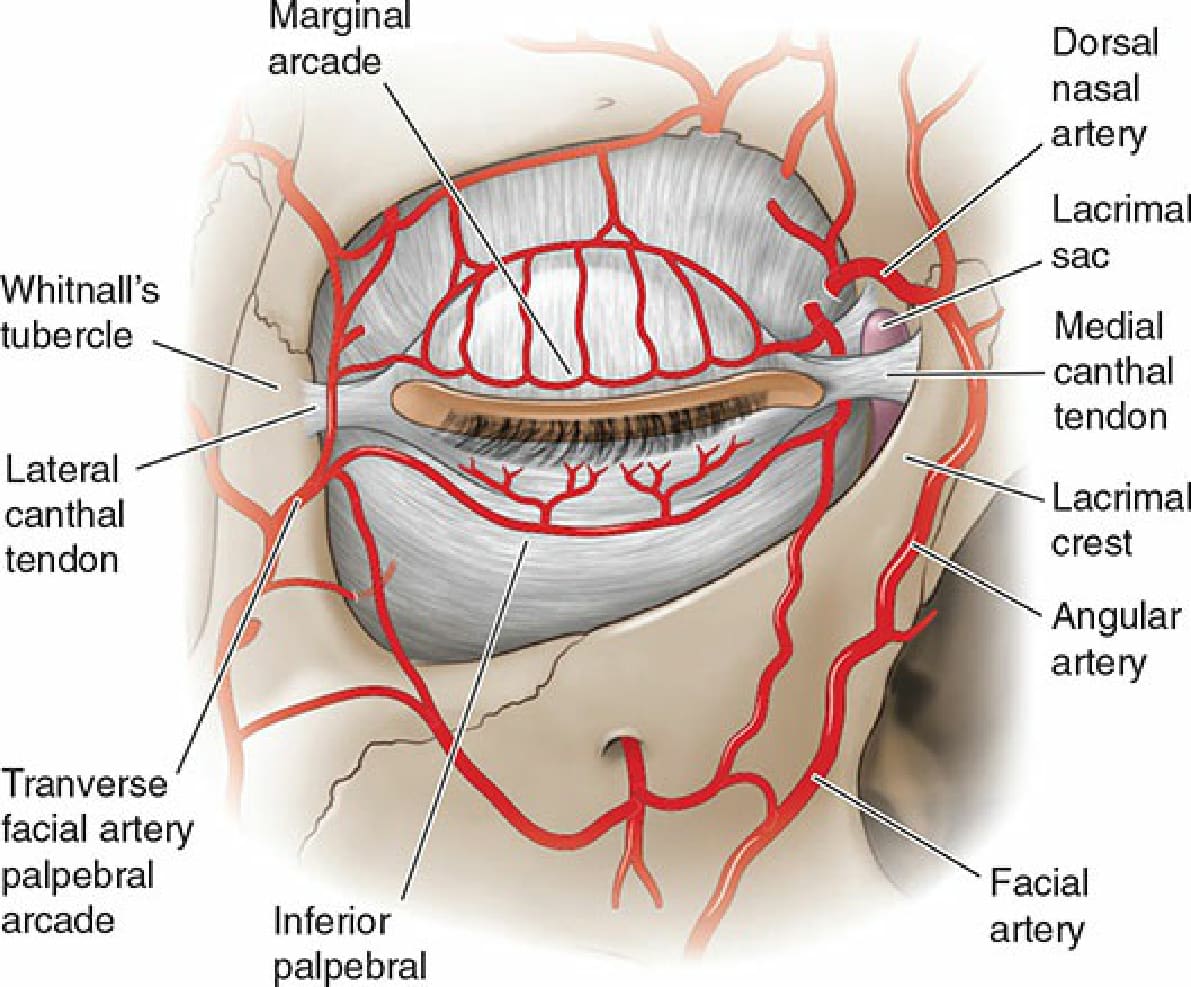
Figure 38-1. Periocular vascular anatomy.