Contact Dermatitis
Contact Dermatitis
ACD represents a type IV hypersensitivity reaction, and ranges in presentation from mildly pruritic erythema to intensely pruritic vesicular, bullous, or indurated plaques. The presence of erythema and induration around a postoperative surgical site may initially raise concern for SSI, but the clinical appearance of a contact dermatitis differs from infection. Contact dermatitis often occurs away from the wound edges, may have an angulated appearance, lacks purulence and tenderness, and is frequently itchy (Fig. 36-12). ACD may be caused by any material in dermatologic surgery, including surgical antiseptics and wound dressings. Antiseptics used to prepare the surgical site are common causes of contact dermatitis. Most commonly, this is seen with povidone– iodine, but a similar reaction has also be reported to chlorhexidine.149 Postoperatively, fixatives (e.g., benzoin and mastisol), dressings (e.g., colophony), and antibiotics (e.g., bacitracin and neomycin) are potential sources of ACD. If a patient has a history of ACD, it is recommended that white petrolatum be used instead of any potential allergyinducing products.149 Contact dermatitis will frequently resolve spontaneously once the implicated agent is removed from the skin. However, in cases of severe reactions that
present with blistering or severe pruritus, topical or even systemic steroids may be helpful.
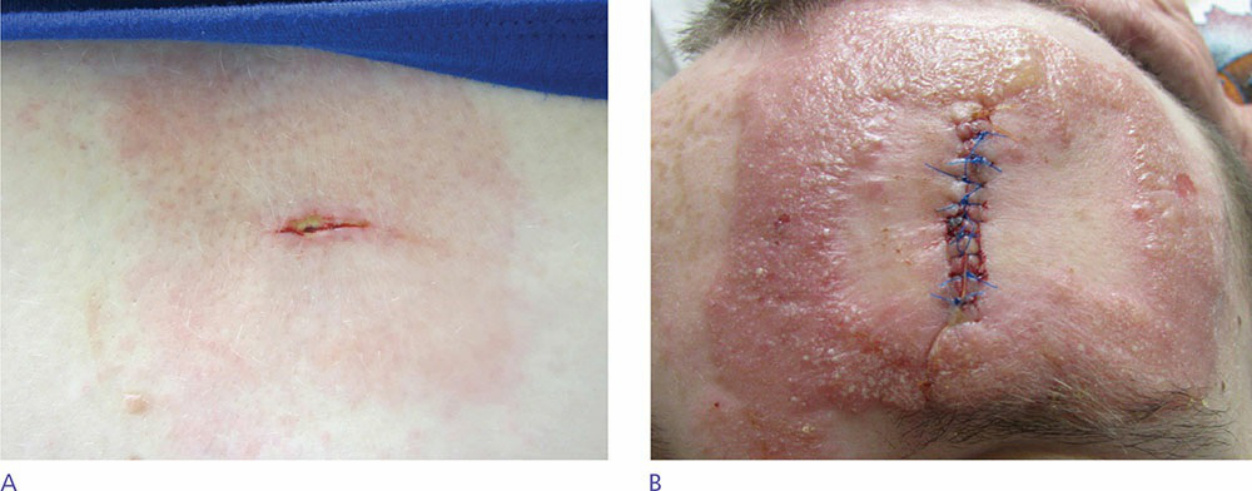
Figure 36-12. Contact dermatitis presenting as angulated erythema corresponding to the location of adhesives. (A) Mild erythema and itching. (B) Severe reaction with blisters and edema.