Antibiotic Prophylaxis
Antibiotic Prophylaxis
Indiscriminant oral antibiotic prophylaxis is discouraged in cutaneous surgery, in light of the risk of possible adverse effects, antibiotic cost, and the potential for contributing to the development of antibiotic-resistant bacteria.107 Antibiotics are associated with numerous adverse side effects ranging from mild gastrointestinal (GI) upset to serious cutaneous reactions such as toxic epidermal necrolysis, acute hepatitis, nephrotoxicity, and Clostridium difficile colitis.108 Not only is the incidence of community acquired MRSA on the rise, but antimicrobial resistance to viridans group streptococci, one of the major causes of infective endocarditis (IE), is also increasingly reported in the literature.108,135
An advisory statement published in 2008 provided an update on the indications for antibiotic prophylaxis in dermatologic surgery for the prevention of SSI, IE, and hematogenous total joint infection (HTJI).114 This statement incorporated recommendations from the 2007 American Heart Association (AHA) guidelines for endocarditis prophylaxis, as well as the 1997 and 2003 American Dental Association (ADA) and American Academy of Orthopaedic Surgeons (AAOS) advisory statements regarding prophylactic antibiotics in preventing HTJI following dental procedures.136–138
If a dermatologic procedure involves the oral mucosa or infected skin (Class II), patients with certain cardiac conditions (Table 36-6) or joint conditions should receive prophylactic antibiotics to prevent IE and HTJI, respectively. High-risk indications for HTJI include a history of total joint replacement within the preceding 2 years, previous prosthetic joint infections, and certain comorbidities with a history of joint replacement at any point in time.114 High-risk comorbidities include insulin-dependent (type I) diabetes, malignancy, immunosuppression, HIV, malnourishment, and hemophilia. Finally, antibacterial prophylaxis may be warranted for high-risk cardiac and whole joint prosthesis patients undergoing dermatologic surgery in sites that are associated with higher rates of infection (below the knee, in the groin, flaps on the ear and nose, wedge excisions, or grafts). These high-risk dermatologic surgery patients may also receive preoperative antibiotic prophylaxis to prevent SSI, but no guidelines exist delineating if and when this is warranted.107
A suggested antibiotic prophylaxis regimen for dermatologic surgical procedures that breach oral mucosa or involve infected skin of high-risk patients is shown in Table 36- 7.114 The same 2008 advisory statement suggested antibiotic prophylaxis regimens for patients at increased risk of SSIs (Table 36-8).114 Finally, in the setting of endocarditis prophylaxis, the AHA advises that an antibiotic should be given 60 minutes prior to a procedure, but may be given up to 2 hours after the procedure, if it is inadvertently not given before the procedure.135 The ADA and AAOS recommended antibiotics to be administered 60 minutes prior to the procedure.114
Treatment Once an SSI is diagnosed, wound culture should be obtained and the patient should be started on empiric antibiotics based on the most likely causal organism. A 7-day course of oral antibiotics is sufficient treatment for most SSIs. In the majority of cases, empiric treatment with an antibiotic that has activity against S. aureus is effective. This treatment includes either a first-generation cephalosporin, such as cephalexin 250 to 500 mg PO three or four times daily, or a penicillinase-resistant penicillin, such as
dicloxacillin 250 to 500 mg PO twice, three or four times daily.117 Antibiotic therapy should be modified, if necessary, based on culture and sensitivity results. If an abscess is present, it should be drained in a sterile setting under LA. Some or all sutures may need to be removed to permit adequate drainage. The wound then may either be packed with sterile gauze or allowed to remain open to drain. The patient should be seen for close follow-up to ensure resolution of the infection and to monitor for future complications.
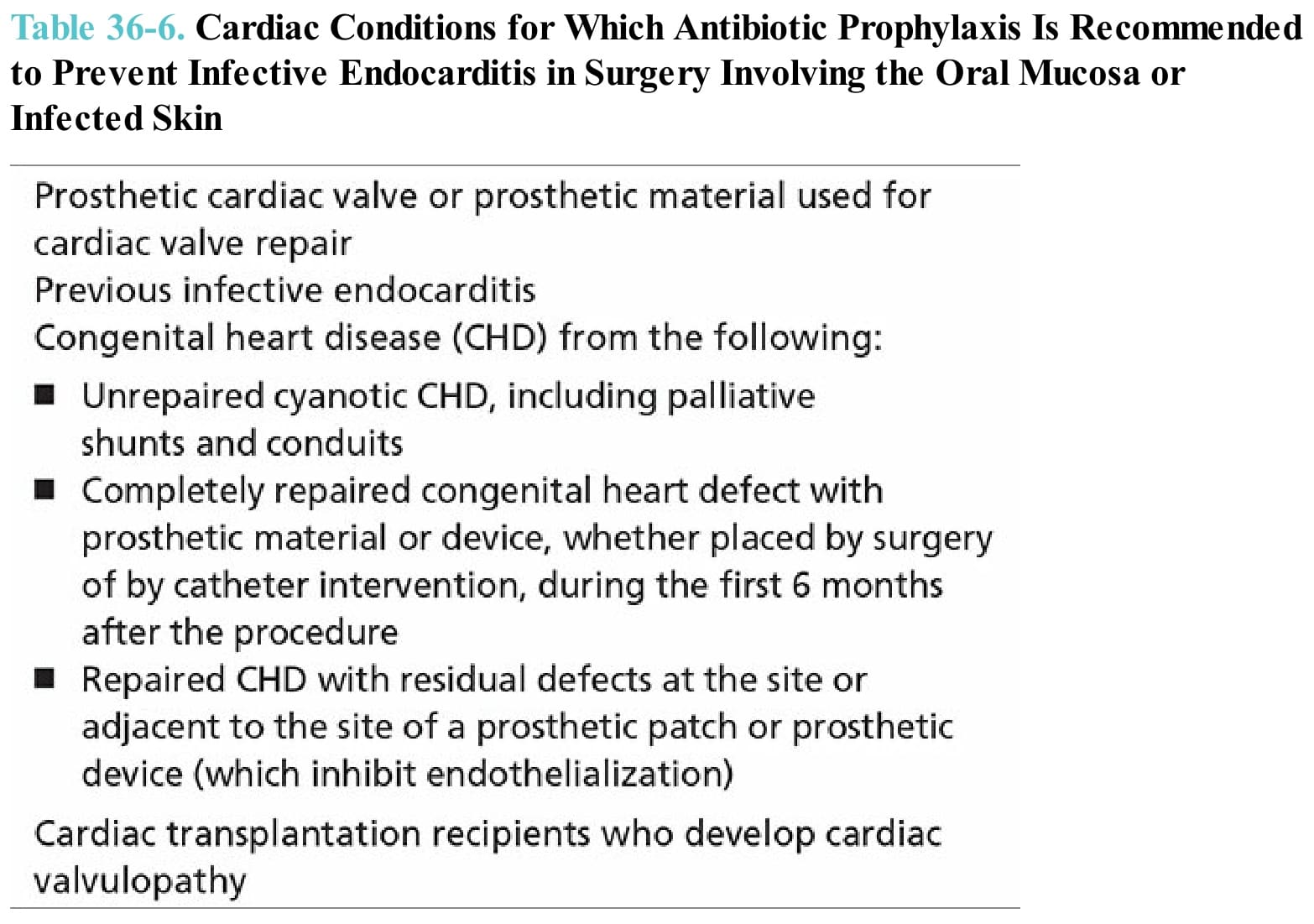
Table 36-6. Cardiac Conditions for Which Antibiotic Prophylaxis Is Recommended to Prevent Infective Endocarditis in Surgery Involving the Oral Mucosa or Infected Skin
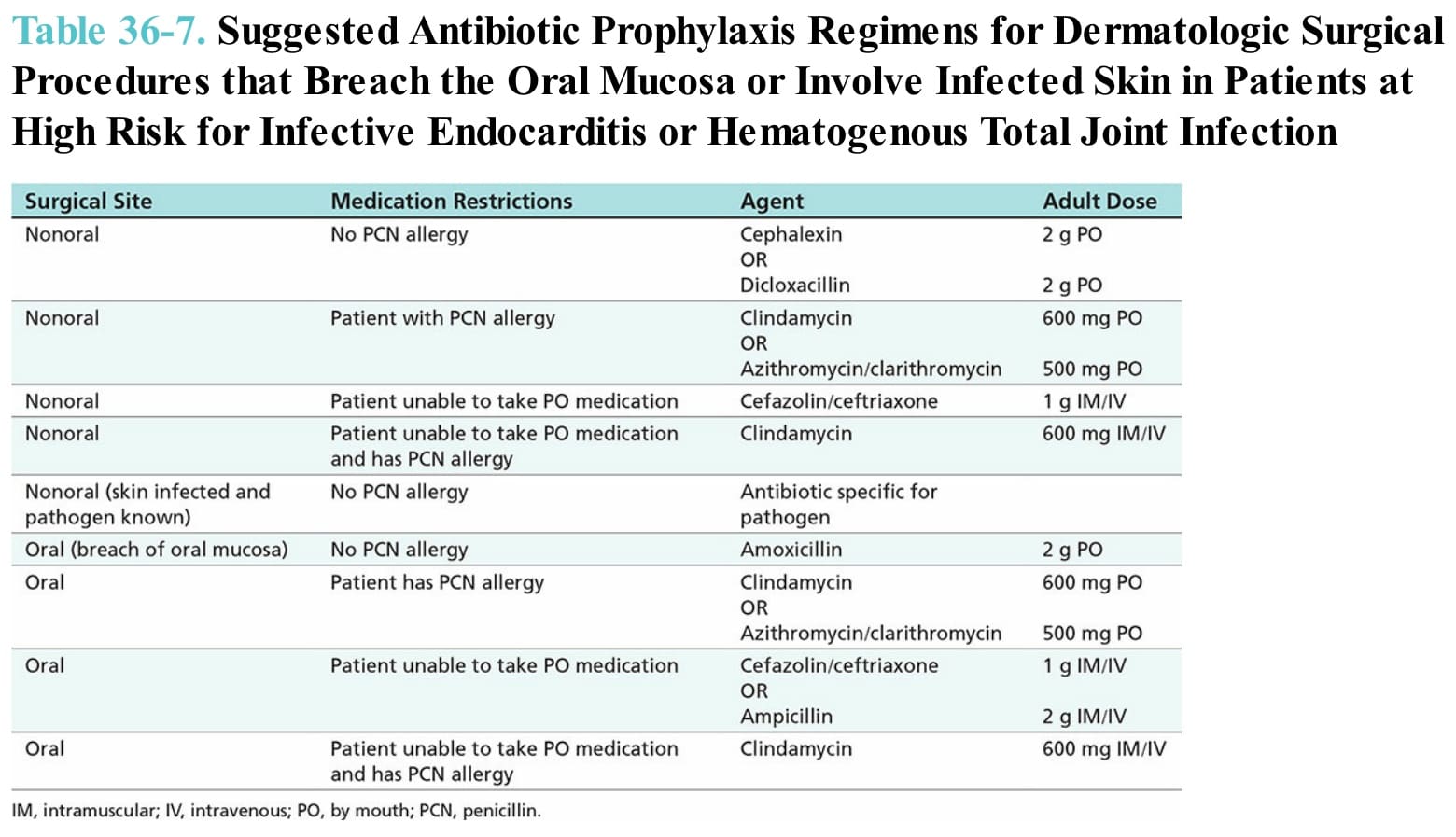
Table 36-7. Suggested Antibiotic Prophylaxis Regimens for Dermatologic Surgical Procedures that Breach the Oral Mucosa or Involve Infected Skin in Patients at High Risk for Infective Endocarditis or Hematogenous Total Joint Infection
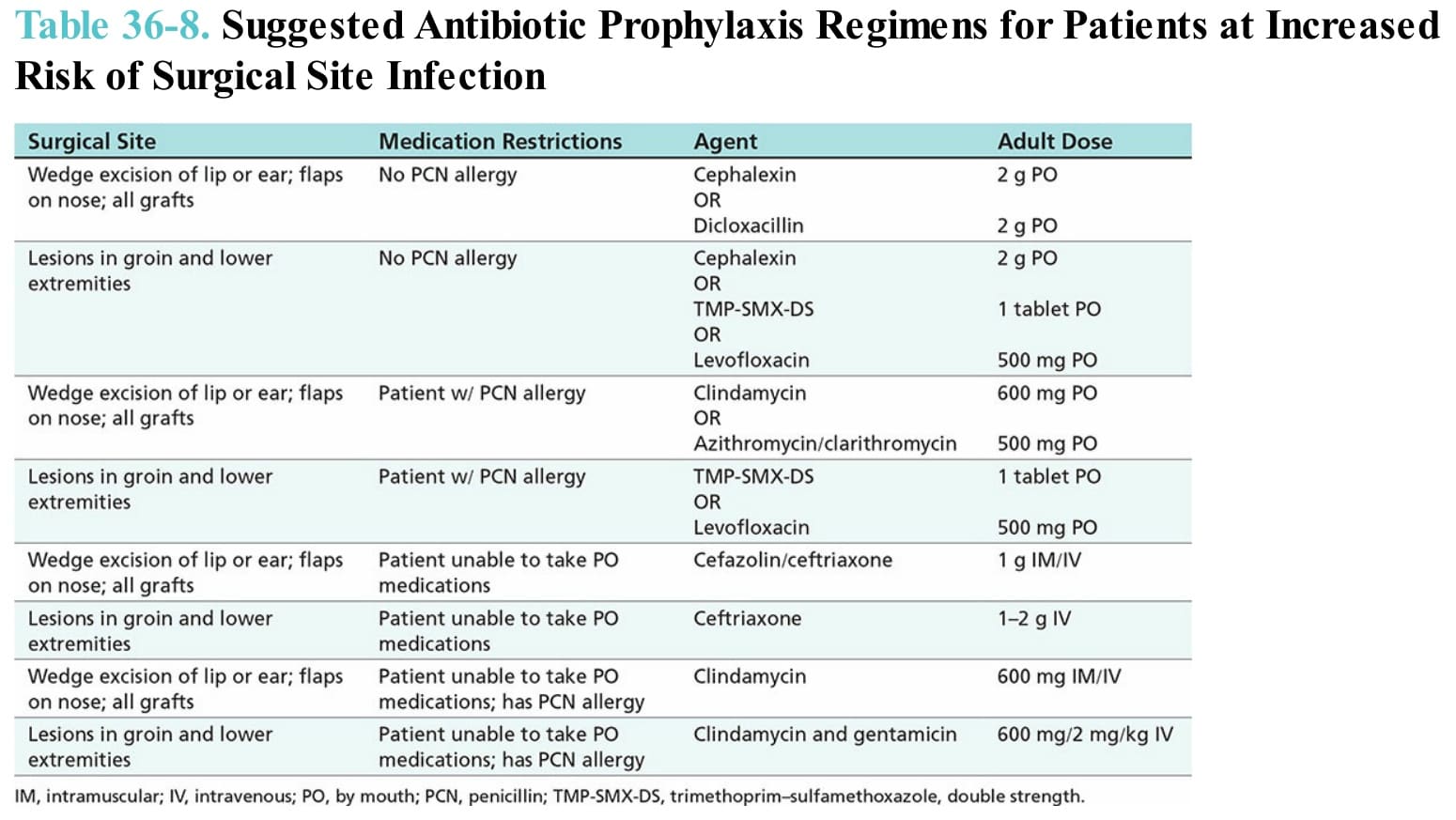
Table 36-8. Suggested Antibiotic Prophylaxis Regimens for Patients at Increased Risk of Surgical Site Infection