Intraoperative Bleeding
Intraoperative Bleeding
Dermatologic surgeons must consider therapeutic antithrombotic medications, herbal supplements, inherited hemorrhagic disorders, and other comorbidities that may place a patient at higher risk of intra- and postprocedural bleeding (Table 36-3).7 Many patients, particularly those undergoing treatment for skin cancer, will have medical conditions that require therapy with anticoagulant and antiplatelet agents. Anticoagulants inhibit thrombin generation and fibrin formation, and include vitamin K antagonists (warfarin), indirect thrombin inhibitors (unfractionated and low–molecular-weight heparins), direct thrombin inhibitors (dabigatran, argatroban, bivalirudin, and lepirudin) and factor Xa inhibitors (rivaroxaban, apixaban, edoxaban, and fondaparinux). Antiplatelet drugs block platelet activation and aggregation, and include aspirin and clopidogrel. Both classes of medications may increase a patient’s risk of intra- and postoperative bleeding, and should be noted prior to the procedure.57,58
Individuals on dual antithrombotic therapy are at the highest risk for procedurerelated bleeding. A 2011 prospective study of 1911 patients demonstrated that patients taking both warfarin and clopidogrel had a 40 times greater risk of bleeding complications compared to other subjects.59 In their retrospective study of 760 patients undergoing skin surgery, another group found a significantly higher rate of bleeding complications in patients taking two or more antithrombotic medications at the time of the procedure.60 In addition to prescription medications, herbal supplements, including ginseng, ginko, vitamin E, fish oil, garlic, dong quai, and others, may potentiate bleeding risks.61–64 Inherited hemorrhagic disorders, including von Willebrand’s disease, hemophilia, and clotting factor deficiencies, should also be identified prior to a dermatologic procedure. These inherited conditions should be managed in conjunction with the patient’s hematologist, given the potential need for premedication or infusions prior to the procedure. Other patient comorbidities, such as uremia, liver disease, excessive alcohol consumption, vitamin K deficiency, immune thrombocytopenia, and bone marrow failure, may further impair thrombosis.7
For patients with increased bleeding risk, pertinent preoperative laboratory data such as prothrombin time (PT)/International Normalized Ratio (INR) and platelet count may be reviewed. Studies suggest that it is safe to proceed with dermatologic surgery if the INR is less than 3.5 within 1 week of the operation.65,66 A platelet count below 50,000 is widely considered a relative contraindication to an invasive procedure. It is recommended to discontinue elective ASA and/or NSAIDS 7 to 10 days before surgery.66 In 2012, the American College of Chest Physicians recommended continuing warfarin or aspirin perioperatively and optimizing local hemostasis during minor dermatologic procedures.67 The current consensus is that individuals should not stop any medically necessary anticoagulants or antiplatelet medications prior to dermatologic surgery, as the risk of catastrophic thrombotic complications exceeds the
risk of bleeding.58,65 There may be instances in which reduction or cessation of anticoagulation is warranted. In such cases, the decision is best made on an individual basis, with active involvement of the prescribing provider.68 A 2015 randomized, double-blind, placebo-controlled study demonstrated that, when patients with atrial fibrillation stopped warfarin therapy prior to an elective procedure, forgoing bridging anticoagulation with low–molecular-weight heparin was noninferior to bridging for the prevention of arterial thromboembolism and resulted in a decreased risk of major bleeding.69 This study indicates that there may be circumstances in which anticoagulation may be stopped without increased risk to the patient.
Consideration of closure type should also be made when operating on patients with an elevated bleeding risk. Of all closure types, flaps, grafts, and partial repairs have the highest risk of bleeding.59 Undermining is important in surgical reconstruction, but should be performed only to the degree necessary to ensure adequate tissue movement. Wide and deep undermining can cause damage to large vessels and result in extensive dead space beneath the closure, thus increasing the risk of bleeding and hematoma formation.7 Drain placement may be appropriate in patients who have a large postoperative wound cavity and/or a baseline bleeding propensity. Drains may be passive or active; passive drains rely on gravity to evacuate fluid, while active drains are attached to a vacuum device. In dermatologic surgery, the drain used most frequently is a passive Penrose drain. The Penrose drain may exit a wound through the inferior aspect of the suture line or from a small opening near the incision. Active drains like Jackson–Pratt (JP) or Hemovacs are closed systems that connect to a reservoir and have the advantage of removing bleeding through negative pressure. Drains should be removed within 24 to 48 hours to minimize the risk of infection (Fig. 36-2).
Management of Uncontrolled Bleeding Intraoperatively Direct pressure over a bleeding vessel for 15 to 20 minutes can tamponade active bleeding, thus allowing physiologic hemostasis to take place. This method is simple and effective, though it prolongs operative time and thus is infrequently utilized.7 In the postoperative period, pressure dressings at the surgical site left in place for 48 hours can reduce the risk of bleeding postprocedure.
Epinephrine is often added to local anesthetics. In addition to improving the duration of action of the anesthetic, epinephrine provides transient vasoconstriction. A recent triple-blinded, randomized control trial found that the time to maximal cutaneous vasoconstriction with lidocaine containing epinephrine 1:1000 is 25.9 minutes.70 One caveat is that some patients may be excessively sensitive to the vasoconstrictive effects of the epinephrine, resulting in an intraoperative pseudo-hemostasis that manifests postoperatively with an increased risk of bleeding or hematoma formation. If this is suspected, meticulous hemostasis of all visible bleeding should take place.7
Suturing techniques may also aid in achieving hemostasis. Occasionally, transection of a larger vessel (>2 mm in diameter) leads to brisk bleeding not amenable to electrosurgery. Suture ligation offers a secure and long-lasting method of hemostasis for these vessels. After identifying the bleeding vessel, both ends of the transected vessel should be clamped with curved hemostats, and each end of the vessel can be directly ligated. Alternatively, in cases where the vessel cannot be directly sutured, a figure-ofeight suture or horizontal mattress suture may be placed around the bleeding area leading to compression and hemostasis.7
Topical hemostatic agents are also commonly used to control intraoperative bleeding. These may be categorized as physical hemostatic agents, chemical hemostatic agents, biologic scaffold hemostatic agents, and biologically active hemostatic agents.71 Physical hemostatic agents function to tamponade blood vessels. Chemical hemostatic agents are caustic and lead to local tissue injury and subsequent thrombus formation. Biologic scaffold hemostatic agents provide a meshwork for platelet aggregation. Biologically active hemostatic agents are purified proteins in the coagulation pathway.7 These materials are listed in Table 36-4. For intraoperative bleeding that will not respond to electrosurgery alone, the most frequently used topical agents are absorbable gelatin (Gelfoam®), oxidized cellulose (Surgicel®), bovine thrombin (Thrombin- JMI®), and recombinant thrombin (Recothrom®).
Electrosurgery is the most commonly used method of hemostasis in cutaneous surgery (Chapter 16). This leads to thermal damage, protein coagulation, and subsequent sealing of bleeding vessels. Electrosurgery includes electrodessication, electrofulguration, electrosection, and electrocoagulation. Another method of hemostasis, electrocautery, does not use electricity but rather direct heat to coagulate bleeding vessels. Electrosurgery and electrocautery are key components of dermatologic surgery, but, when used in excess, can result in delayed wound healing and poor cosmesis due to thermal tissue damage and injury to the surrounding lymphovasculature.7

Figure 36-2. (A) Penrose drain placed in a large flap closure. This passive drain needs to be placed at the most inferior aspect of the wound. (B) Jackson–Pratt drain placed in a large flap closure.
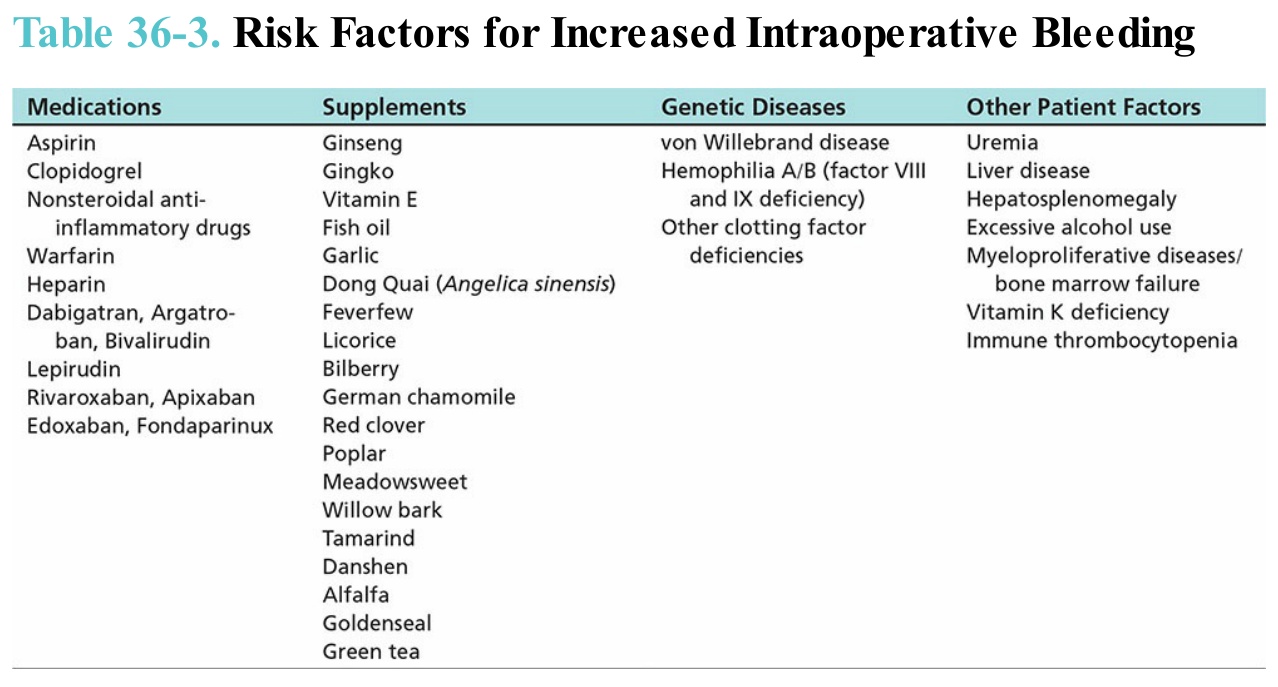
Table 36-3. Risk Factors for Increased Intraoperative Bleeding
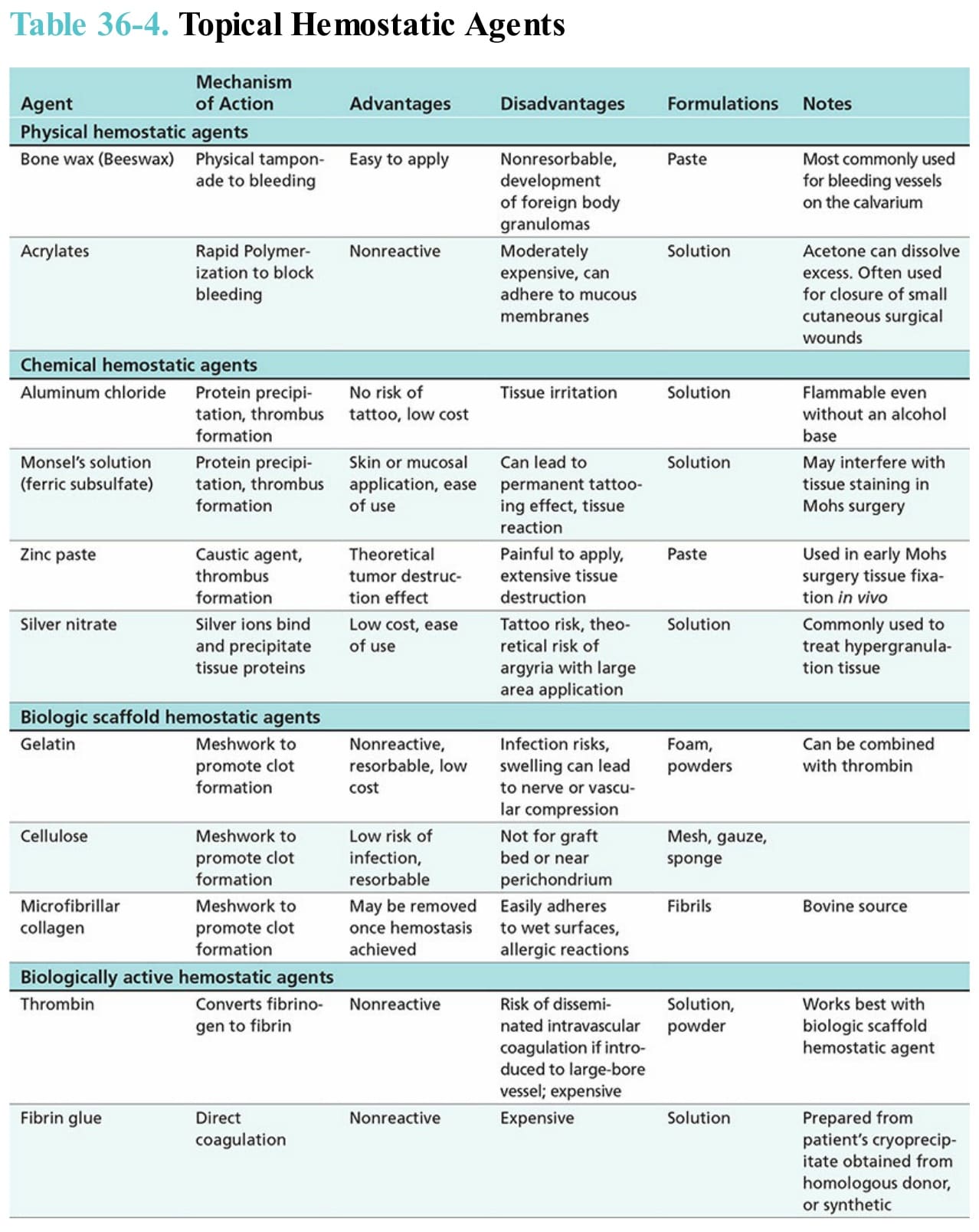
Table 36-4. Topical Hemostatic Agents