Allergy/Anaphylaxis
Allergy/Anaphylaxis
A rare but important side effect of LAs is allergic reaction. These reactions involve either type I (immediate) or type IV (delayed-type) hypersensitivity. Most true allergic reactions to LAs are type IV reactions, also known as contact allergy. A retrospective chart review of 1819 patients found that type IV hypersensitivity to LAs has been increasing, with benzocaine (45%), lidocaine (32%), and dibucaine (23%) as the most common allergens.31 This phenomenon is thought to be due to an increased number of over-the-counter products containing lidocaine, resulting in unnecessary exposure and sensitization. Type IV hypersensitivity results in a local eczematous dermatitis, characterized by erythematous papules and/or vesicles that may progress to plaques and bullae; anaphylaxis is not a risk.31,32 The time course of type IV hypersensitivity is most commonly at least 48 hours after exposure.
In contrast, type I reactions are IgE-mediated and occur minutes to hours after exposure to an antigen. Local manifestations of type I hypersensitivity are isolated urticaria or angioedema without laryngeal involvement. Systemic manifestations, or anaphylaxis, include bronchospasm and peripheral vasodilation, presenting as tachycardia and hypotension (Table 36-1). Overall, the rate of true IgE-mediated allergy to LAs in very high-risk populations (patients reporting an LA allergy) has been found to be around 1%.32 Thus, the prevalence of IgE-mediated LA allergy in the general population is presumably significantly lower. While latex, found in surgical gloves, was previously one of the most common causes of anaphylaxis in the medical setting, widespread efforts to reduce latex exposure and sensitization have resulted in a marked decrease of the number of reactions.33 Reports of anaphylaxis due to antibiotics, dyes, and chlorhexidine have been increasing in frequency.33
There are two classes of commercially available LAs: amides and esters. True type I allergy to amide anesthetics, including lidocaine and bupivacaine, is exceedingly rare. Most true LA allergies have been reported with ester anesthetics, including procaine, tetracaine, and benzocaine. The ester anesthetics more commonly elicit an allergic reaction because they are p-aminobenzoic acid (PABA) derivatives. There is no crossreactivity between amide and ester anesthetics, but the preservative methylparaben, used as a stabilizer in multiple-dose vials of lidocaine, is structurally related to PABA. Thus, PABA and other preservatives, including sodium metabisulfite, are likely the most common cause of a reported allergy to amide LAs.34–36 Single-dose vials of lidocaine are available without preservatives.
If a history of type I LA allergy is documented, patients can be referred to an allergy specialist for evaluation. If an LA allergy is reported but considered low risk based on patient history, an intradermal or subcutaneous challenge can be performed in the office. This assessment is performed by injecting into the skin a 2- to 3-mm superficial bleb of a 1:1000 dilution of an LA (without epinephrine) from the opposite class as the suspected allergen. In addition, a positive control (0.10 mg/mL of histamine base) and negative control (normal saline) should be injected for comparison. The wheal and flare reaction should be evaluated at 15 to 20 minutes and, if the longest diameter of the wheal is at least 3 mm greater than the negative control, the test is considered positive. If the result of the 1:1000 dilution is negative, an increased concentration of 1:100 should also be tested before deeming the test negative. If negative, a subcutaneous challenge can then be performed with an undiluted concentration of LA.32
It is important to be able to differentiate an anaphylactic reaction to LA from the much more common vasovagal and epinephrine reactions, which are frequently interpreted by patients as an “allergy” to LA. When a patient has systemic symptoms after the administration of an LA, a set of vitals should be taken, as well as a thorough review of systems.
With true anaphylaxis, tachycardia is coupled with hypotension. The patient may have bronchospasm, urticaria, angioedema, or other systemic symptoms such as nausea, vomiting, and diarrhea. Intramuscular epinephrine should immediately be given for anaphylaxis and the threshold for administration should be low. Treatment with antihistamines or steroids is inappropriate in cases of suspected anaphylaxis. The recommended dosing for an adult is 0.3 to 0.5 mg (this typically equals the same volume: 0.3 to 0.5 mL of a 1 mg/mL solution) of a 1:1000 solution delivered intramuscularly. This injection may be repeated every 5 minutes as needed. For a child, the recommended dosing is 0.01 mg/kg up to the adult dose of 0.5 mg. Commercially available auto-injectors deliver a preset dose of epinephrine. Dermatologic surgeons should have epinephrine solution or epinephrine auto-injectors readily available to treat suspected anaphylaxis.
If the patient is having a benign reaction to epinephrine, tachycardia with hypertension is expected. The most commonly used concentrations of epinephrine in dermatologic surgery are 1:100,000 and 1:200,000 for LA and 1:1,000,000 to 1.5:1,000,000 for tumescent anesthesia.37 Even the low concentrations of epinephrine in these formulations can cause systemic effects, such as palpitations, flushing, and a feeling of panic. Epinephrine effects typically resolve spontaneously and usually do not require treatment. If needed, the recommended treatment is a non-selective betablocker.32 Patients can interpret the epinephrine response as anxiety or a cardiac complication, so it is important to provide reassurance as to the benign and temporary nature of this reaction. Epinephrine should be avoided in patients who have a medical
history of uncontrolled hyperthyroidism or pheochromocytoma.32 Local infiltration with epinephrine has been used safely for dermatologic procedures in patients with stable cardiovascular diseases including hypertension, ischemic heart disease, arrhythmia, coronary artery disease, and heart transplantation. If there is any concern about a patient’s ability to safely undergo a procedure due to cardiovascular disease, the patient’s cardiologist should be consulted.37
In a vasovagal reaction, bradycardia and hypotension are typically seen. This will be the most commonly encountered scenario in clinical practice. Vasovagal reaction is due to the activation of the vagus nerve in response to anxiety, fear of needles, or pain on injection, and results in heightened parasympathetic tone.38 The patient will likely describe sweating, nausea, and hyperventilation.32 Patients may feel like they are about to lose consciousness (presyncope) or lose consciousness (syncope). Patients who experience syncope may lose bladder control and have rhythmic movements that can mimic a grand mal seizure.39 One study revealed that young patients are more likely to experience presyncope compared with older patients, and that young males are most prone to develop true syncope.40 If the patient is having a vasovagal response, reassurance, placing a cool towel on the forehead, and placing the patient in Trendelenburg can alleviate the symptoms. For vasovagal reactions not responding to these measures, atropine 0.4 mg delivered subcutaneously can be considered.32 Given the risk of vasovagal reactions, it is helpful to always infiltrate LA with the patient in a supine position.
Overdose Life-threatening systemic toxicity can potentially occur when LAs exceed their maximum dosage, or when excretion is impaired. Lidocaine has a maximum, weightbased dose of 4.5 mg/kg without epinephrine and 7.0 mg/kg with epinephrine.37 Lidocaine toxicity is rare in dermatologic surgery; a 2010 study demonstrated that perioperative peak lidocaine levels during MMS do not result in serum levels approaching toxic limits, even when relatively high total lidocaine doses (up to 50 mL) are used.41 Despite this finding, toxicity has been reported as a complication of dermatologic surgery, and it is important for dermatologic surgeons to be aware of the signs, symptoms, and management of LA toxicity.42,43 Inadvertent intravascular administration of local anesthetic may cause systemic toxicity more commonly than gross excess of infiltrated anesthetic.42,43
Overdose of lidocaine results in CNS toxicity and cardiovascular toxicity due to decreased cardiomyocyte contractility (Table 36-2). Initial signs and symptoms of lidocaine overdose occur at blood concentrations of 1 to 6 μg/mL and include perioral and digital numbness or tingling, restlessness, and lightheadedness. The patient may be increasingly talkative and describe a metallic taste in their mouth. At a concentration of
6 to 9 μg/mL, the patient may experience nausea, vomiting, twitching, tremors, blurred vision, tinnitus, and confusion. While the patient may still have a normal pulse and blood pressure, consider treating with benzodiazepines or barbiturates and ensure the airway is patent. At a blood concentration of 9 to 12 μg/mL, seizures may occur. Anticonvulsants may be used prophylactically in this situation. Additionally, initial manifestations of cardiovascular compromise may be seen, with the patient having lower than normal pulse and blood pressure. At >12 μg/mL blood concentration, the patient is at risk of coma and cardiopulmonary arrest.44
Bupivacaine has a maximum, weight-based dose of 2.5 mg/kg without epinephrine and 3.0 mg/kg with epinephrine.37 Of the non-lidocaine LAs, bupivacaine exhibits the smallest therapeutic range. Acutely elevated plasma levels may result in ventricular tachyarrhythmias and asystole, even before CNS symptoms develop.44 If there is any concern for LA overdose of any type, anesthesia administration should be stopped and vital signs obtained. Dermatologic surgeons should have a low threshold for a transfer to a higher level of care in these cases, given the potential morbidity and mortality of anesthetic toxicity.
Digital Anesthesia There is a historically entrenched belief that epinephrine can cause tissue ischemia and necrosis due to vasoconstriction of end arteries via alpha-1 receptors, particularly of the digits.45 In recent years, research and reviews have invalidated this doctrine, and current evidence demonstrates that LA with epinephrine is safe for use in all clinical locations, including the digits. One study demonstrated no digital necrosis using 0.5% lidocaine with epinephrine 1:200,000 for digital anesthesia in 63 cases, including patients with peripheral vascular disease, hypertension, and diabetes mellitus.46 Another study examined patients who accidentally injected themselves with an
epinephrine pen used for anaphylaxis. No cases of digital gangrene were noted, and the epinephrine concentrations used in epinephrine auto-injectors are much higher than those used in LA for cutaneous surgery.47 Phentolamine is a reversible nonselective alpha-adrenergic antagonist recommended for epinephrine-induced digital vasospasm, although its use after dermatologic surgery has not been reported.48–51
Digital blocks can be safely performed with LA with epinephrine. The surgeon should avoid using more than 2 to 4 mL of anesthesia per digit, as the mass effect of the LA volume can potentially lead to nerve and artery compression. Circumferential ring blocks should also be avoided for this same reason.52 It is important to note that tubular dressings, rather than epinephrine or large volumes of LA, are the most common cause of iatrogenic digital ischemia and necrosis, due to a tourniquet effect.53–56

Table 36-1. Distinguishing Reactions to Local Anesthetics in Dermatologic Surgery
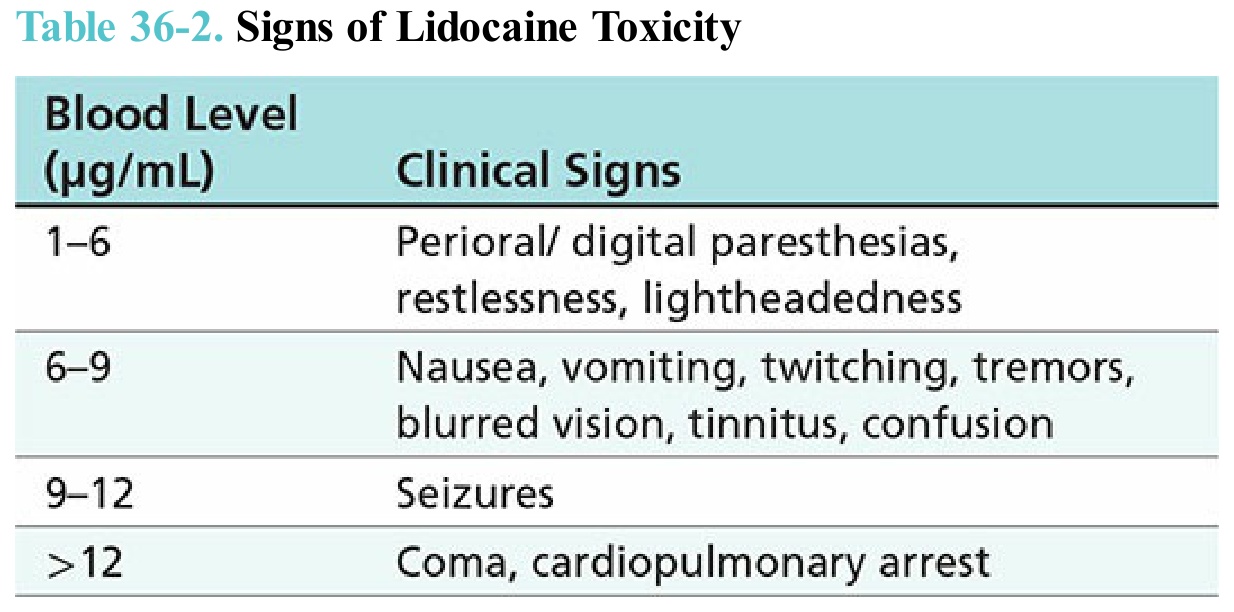
Table 36-2. Signs of Lidocaine Toxicity