SURGICAL TREATMENT
SURGICAL TREATMENT
Fusiform excision is the most basic technique for surgical scar revision. The entire length of the scar is excised with as narrow a margin as possible resulting in a longer— and ideally narrower—scar (Fig. 35-3).1 Such revised fusiform excisions generally have a length-to-width ratio well in excess of 3:1, with 30-degree angles at the apices. In lieu of complete scar excision, partial removal can alternatively be performed, as in the case of the standing cone revision (Fig. 35-4). Table 35-3 is a summary of surgical approaches to scar revision.
Z-plasty is another commonly employed technique that reorients the direction and tension vectors of a scar, allowing it to be aligned within RSTLs (Fig. 35-5).38 It is indicated for webbed scars, contracted scars, and scars that are greater than 30 degrees from the RSTLs.39 In this technique, the original scar forms the common diagonal, and two arms of equal length to the original scar are extended in either direction at a set angle.40 The original scar is then excised, with incisions made along arms of the Z, with subsequent undermining and transposition of the two triangular flaps to create a new scar perpendicular to the original one. The size of this angle and the length of the original scar determine how much scar lengthening will occur when the tension is redirected, with larger angles producing a greater lengthening in the scar as well as a
greater reorientation of the direction of the scar. The traditional angle of 60 degrees lengthens the scar by 75%. Multiple Z-plasties may also be used in succession for longer scars. For a detailed discussion of Z-plasty techniques, see Chapter 27.
In comparison, the W-plasty technique does not result in the lengthening of the original scar and involves the creation of multiple, short, connected, triangular advancement flaps that run along the length of the original scar (Fig. 35-6). This technique is often employed for shorter scars located on the forehead or cheek with an M-plasty at the end of the incision to prevent scar extension.41 Additionally, in comparison to the Z-plasty which involves excision of the scar and incisions along the arms, the W-plasty involves the excision of the scar and a small amount of surrounding normal skin.39 A more complex variation of the W-plasty is a geometric broken line closure in which a random pattern of geometric patterns is interposed in order to create a random irregular scar.39,41
A V–Y advancement flap may be used at free margins such as the lip or eyelid in order to correct contraction which may result in elevation or depression of the tissue.40
This technique may be used to correct ectropion on both the upper and lower eyelids.42 A V-shaped incision is made surrounding the contracted scar, with wide undermining performed circumferentially. This V-shaped pedicle is then pushed forward by side-toside closure of the tail of the Y posterior to the now-advanced pedicle, altering the tension on the contracted scar and allowing for an improved cosmetic outcome (Fig. 35-

Figure 35-3. Scalpel revision for disunion of the nasal tip. (A) Preoperative view following referral for disunion at nasal tip following graft failure. (B) Postoperative view following excision of scar and primary closure.

Figure 35-4. Scalpel revision of standing cone. (A) View at closure of defect from Mohs for incompletely excised BCC on the lip. (B) Standing cone on inner lower lip covered teeth with full smile. (C) Immediate postoperative view following excision of standing cone.
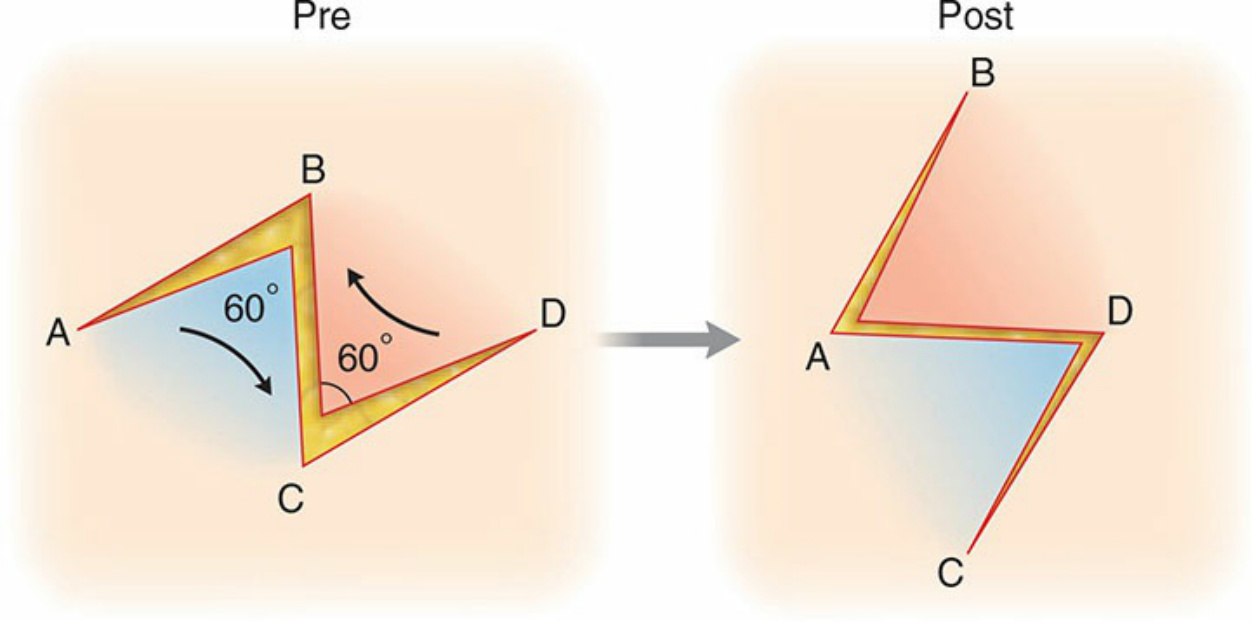
Figure 35-5. In a Z-plasty, two arms of equal length to the original scar are extended in either direction at a given angle. The original scar is then excised with incisions made along these arms followed by transposition of these two triangular flaps to create a new scar that is perpendicular to the original one. This results in scar lengthening and is thus useful for correction of webbing and free margin distortion.
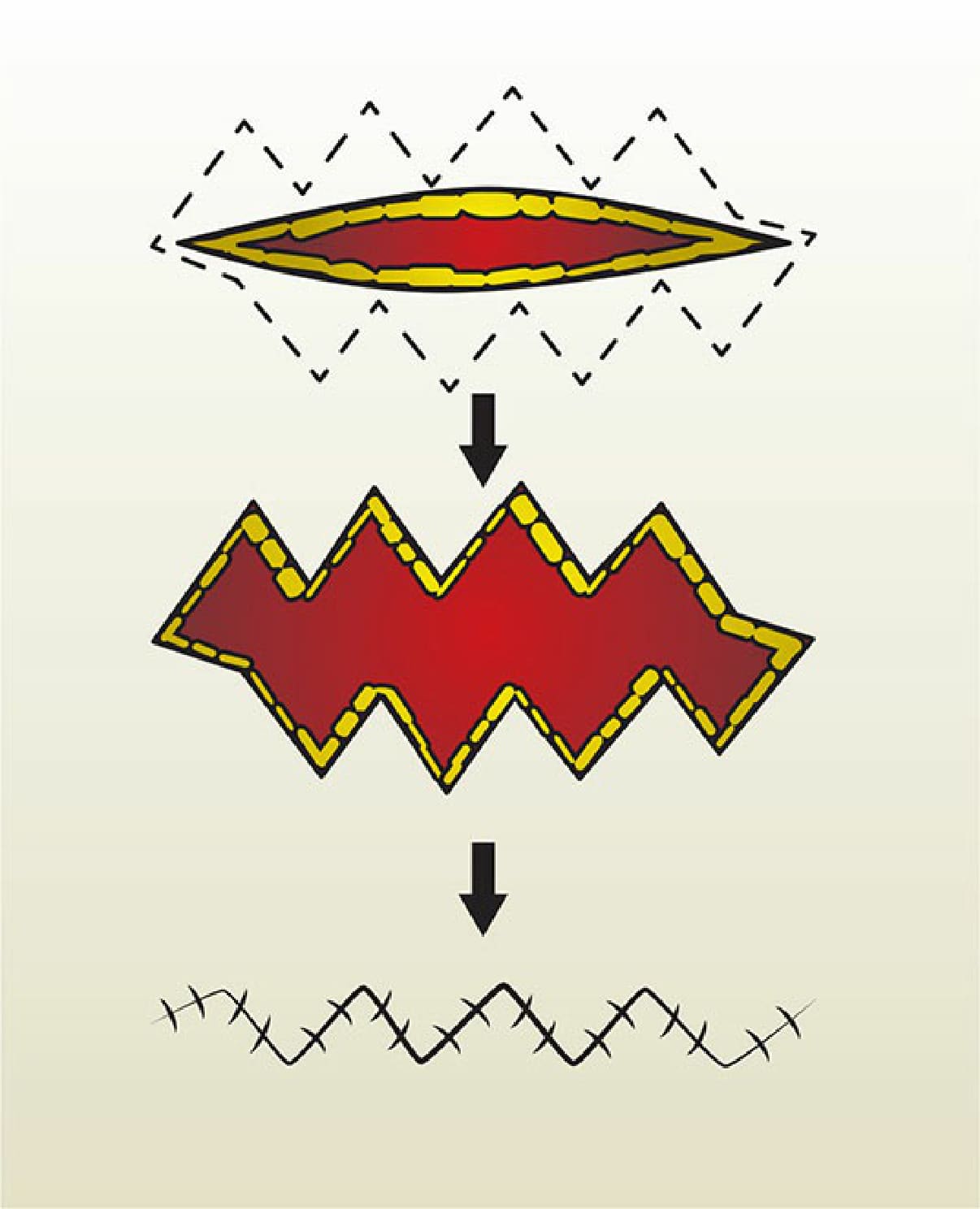
Figure 35-6. W-plasty technique involves the creation of multiple, short, connected, triangular advancement flaps that run along the length of the original scar. This does not result in lengthening of the scar as is the case with Z-plasty.
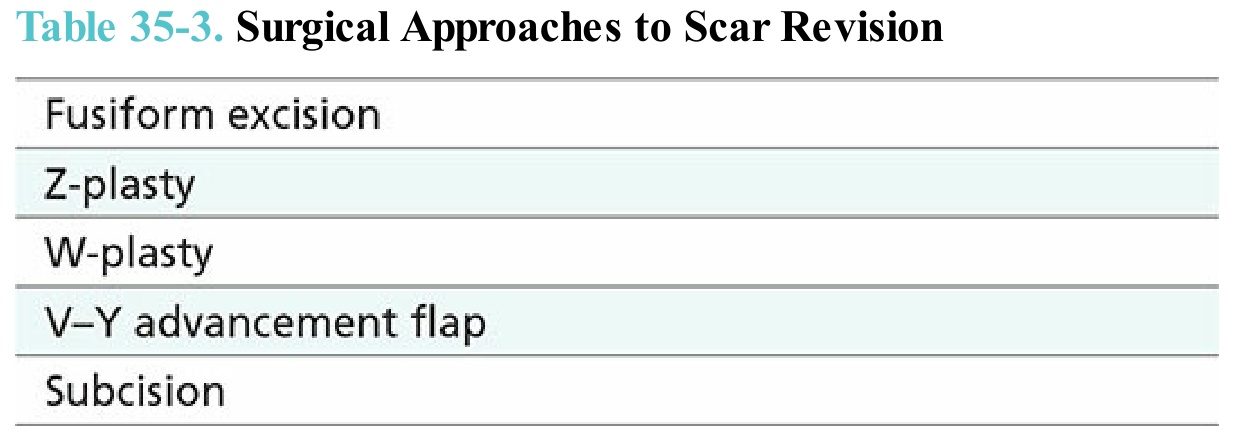
Table 35-3. Surgical Approaches to Scar Revision