LASER- AND LIGHT-BASED APPROACHES
LASER- AND LIGHT-BASED APPROACHES
The original 2002 scar management consensus guidelines addressed CO2 lasers, argon lasers, and pulsed-dye laser (PDL) therapies. Since then, numerous other therapies have emerged including ablative and nonablative fractional lasers. Table 35-2 is a summary of minimally invasive approaches to scar revision.
The 585-nm PDL was the first laser to gain wide acceptance for use in treating scars postoperatively.4,9 The PDL targets oxyhemoglobin as its chromophore, and is effective in targeting small blood vessels within scar tissue, improving erythema. This approach may also be used after superficial flap necrosis (Fig. 35-2). Additionally, PDLs have been used for hypertrophic scars and keloids, leading to possible improvement in scar pliability.9 While the exact mechanism of action has yet to be elucidated, it is postulated that microvascular destruction and tissue ischemia may lead to collagen remodeling, and that PDL treatment may reduce the higher levels of transforming growth factor-beta which is found in keloids.10,11 Sub-purpuric settings with longer pulse durations and lower fluences may demonstrate superior outcomes to purpuric settings in surgical scars, though both are effective.10,11 Adverse effects include erythema, swelling, ecchymoses, and hypopigmentation. Alternatively, the 532-nm potassium titanyl phosphate (KTP) laser or intense pulsed light (IPL) may also be used for erythema in surgical scars.
Introduced in 1953, dermabrasion is another useful modality for treating surgical scars.12 Dermabrasion is often performed 4 to 8 weeks postoperatively when tissue remodeling is taking place, though it may also be used significantly later.13–15 The most common adverse effects include hypo- and hyperpigmention, persistent erythema, infection, viral reactivation, and rarely keloid formation. Following dermabrasion, ablative resurfacing with high-energy, short-pulsed CO2 lasers or low-power
continuous-wave CO2 lasers was popular as an effective means of skin resurfacing, though they have significant healing time and postoperative wound care.16–18 In comparison to dermabrasion, ablative CO2 lasers offer the advantage of a bloodless field and increased precision with more selective tissue ablation.19 However, patients experience crusting, oozing, and often persistent erythema with re-epithelization at approximately 1 week and erythema persisting for 4 to 8 weeks. Adverse effects include hypo- and hyperpigmentation, milia formation, infection, viral reactivation, and scarring.
More recently, fractional ablative and nonablative laser resurfacing has been used with increasing frequency for scar revision. In fractional resurfacing, the laser creates microthermal zones (MTZs) of injury just below the skin surface, with selective necrosis and neocollagenesis.20 This technology specifically spares the tissues surrounding each individual microscopic wound, which allows for faster healing and less downtime. The 1550-nm erbium-doped fiber laser, which utilizes nonablative fractional resurfacing, was shown to be effective in surgical scars.21 In a split-scar study comparing nonablative fractional resurfacing with PDL following Mohs micrographic surgery, nonablative fractional resurfacing showed improved outcomes for overall cosmesis, dyspigmentation, hypopigmentation, thickness, and texture of scar.22 The most common posttreatment events include dry and flaking skin, erythema, edema, acneiform eruption, and viral reactivation, with healing occurring within 1 week.23,24 Ablative fractional resurfacing has been used as well.25,26 Sparing surrounding areas of tissue, ablative fractional resurfacing allowed for re-epithelization and resolution of erythema within 7 days, with deeper zones of tissue ablation.26,27 Ablative fractional resurfacing may be more effective than nonablative fractional resurfacing, and has shown utility in thicker and atrophic scars.1,27,28 A small series of atrophic scars showed that three ablative fractional resurfacing treatments at 1- to 4- month intervals resulted in a 38% mean reduction in scar volume and 35.6% mean reduction in maximum scar depth.27 In comparison to PDL, which is more effective at improving vascularity within scars, ablative fractional resurfacing demonstrates superior results in improving scar contour, including scar thickness and pliability.29 In a postthyroidectomy surgical scar study comparing fractional ablative laser resurfacing to nonablative fractional laser resurfacing, fractional ablative laser resurfacing tended to improve scar thickness, while nonablative fractional laser resurfacing was superior at improving scar color including erythema and pigmentation.30,31 This benefit should be weighed against the increased downtime seen with ablative approaches.
Finally, microneedling and microneedle fractional radiofrequency have also been used to improve the functional and aesthetic outcomes of surgical scars. Subcision, with the insertion of a needle through punctured skin for the correction of depressed scars,
was first reported in 1995.32 A small randomized clinical trial comparing nonablative fractional laser and microneedling in atrophic acne scars showed both to be efficacious, with microneedling having fewer adverse effects including hyperpigmentation.33 Microneedling has also been shown to increase the viability of skin flaps in animal models, though there are no reported studies of its efficacy in the treatment of surgical scars to date.34 Currently on the horizon, radiofrequency microneedling has also been shown to improve acne scars by damaging the reticular dermis, resulting in tissue remodeling and the increased formation of elastin and collagen.35–37

Figure 35-2. PDL for telangiectasia and erythema after flap necrosis. (A) Defect after cancer removal. (B) Rotation flap repair. (C) Distal necrosis at suture removal. (D) Result after conservative wound care and three treatments with PDL.
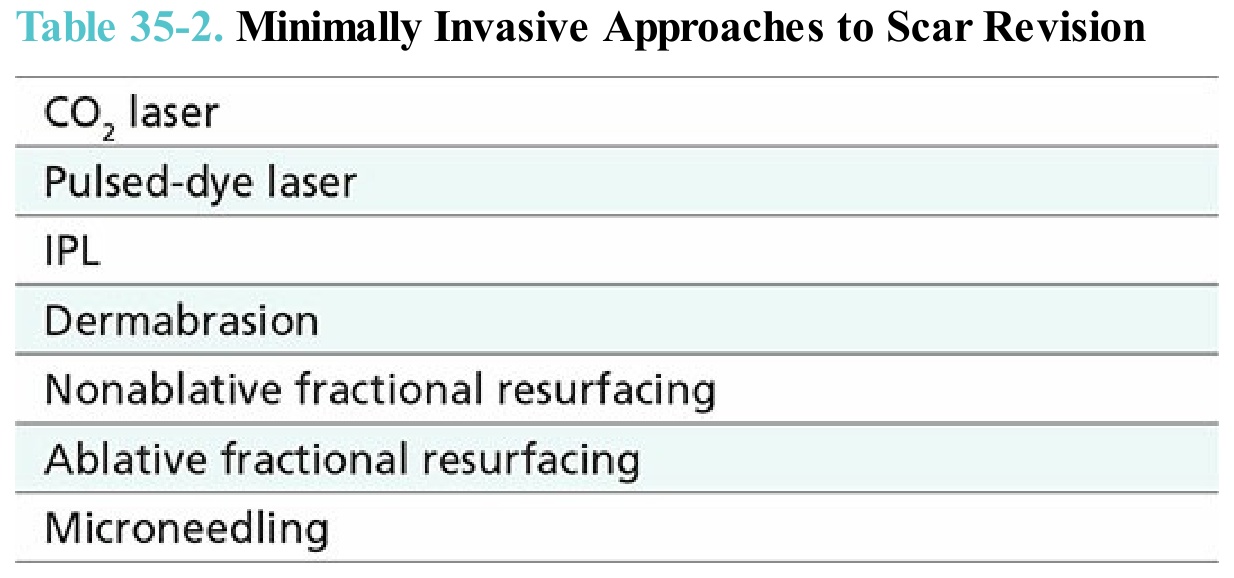
Table 35-2. Minimally Invasive Approaches to Scar Revision