INTRALESIONAL APPROACHES
INTRALESIONAL APPROACHES
Intralesional corticosteroids are the mainstay of treatment for hypertrophic and keloidal scars.2,5 Injection of triamcinolone acetonide has been an evidence-based approach
since 1966 when the first controlled study of its use was reported.6 Used in concentrations ranging from 10 to 40 mg/mL, it can also be combined with intralesional 5-fluorouracil (5-FU), laser therapy, or surgical intervention with injection at the time of treatment to prevent keloidal scar formation (Table 35-1). Adverse effects of intralesional corticosteroid injection include atrophy, telangiectasia, and hypopigmentation.
In 1999, Fitzpatrick reported on nine clinical years of experience of injection of 5- FU for the treatment of hypertrophic and keloidal scars.7 Patients were treated with 5- FU at a concentration of 50 mg/cc with doses ranging from 2 to 50 mg per treatment with injections occurring up to three times weekly, with reduction in frequency to every 4 to 6 weeks following the improvement of scars. He also combined 0.9 cc of 5-FU at 50 mg/cc and 0.1 cc of triamcinolone acetonide at 10 mg/cc and found these injections to be less painful. Re-excision of keloids with intraoperative intralesional 5-FU and/or triamcinolone is also highly effective (Fig. 35-1).8 Patients who are pregnant or immunosuppressed should not be injected with 5-FU.
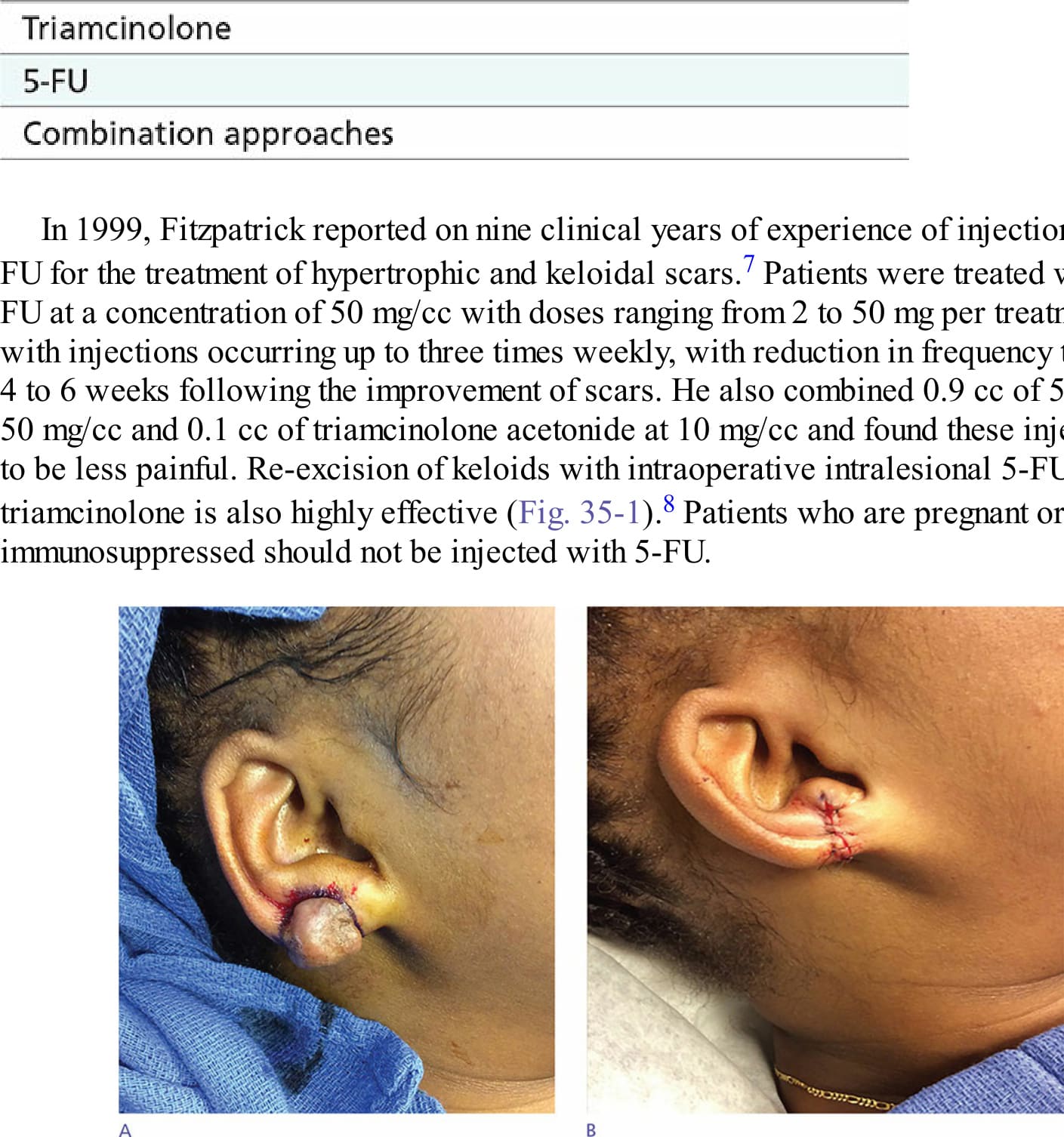
Figure 35-1. Removal of keloid followed by injection of triamcinolone plus 5-fluorouracil: (A) preoperative view; (B) postoperative view. Patient underwent monthly injections of triamcinolone and 5-fluorouracil for 4 months.
Table 35-1. Intralesional Options