POSTOPERATIVE CONSIDERATIONS
POSTOPERATIVE CONSIDERATIONS
Surgical planning includes anticipation of and preparation for postoperative considerations. Patients leave the clinic with a padded bandage in place (Fig. 34-22). An in-office dressing change at 48 hours postoperatively should be offered and, while some patients appreciate this, most patients choose instead to change the dressing at home. Written instructions are provided.
Pain management is an important concern after surgery. It is important to stress to patients that elevation of the surgical site and following activity restrictions are important parts of pain prevention. For punch and tangential biopsies and phenolization, acetaminophen for the first 48 hours is adequate. Total nail avulsion is painful, and for the first 48 hours, narcotic pain medication may be prescribed. For lateral longitudinal excisions, flaps, and grafts, narcotics are almost always needed. It is not unusual for patients to only need analgesics for the first 24 hours after a light and limited nail surgery.
COMPLICATIONS
All surgical procedures have risks.26 These include pain, bleeding, infection, scarring, dysesthesia, implantation cysts, necrosis, recurrence and nondiagnostic biopsy. Careful surgical planning and thorough patient education limit the complications of nail surgery. Patients undergoing nail surgery should be informed of the risks of nerve damage and permanent nail dystrophy. Complications remain extremely unusual in the hands of experienced surgeons.
Postoperative pain is minimized with the replacement of the nail plate after surgery, with instructions for the patient to keep the digit elevated and limit activity for 48 hours after surgery, and by anticipating pain with adequate analgesics.
Bleeding is the most common complication of nail surgery, and occurs when the tourniquet is removed. Anticoagulants and antiplatelet agents should not be interrupted prior to nail surgery, as the risks from stopping those drugs outweigh the potential benefit.
For moderate bleeding, oxidized cellulose or calcium alginate dressings work nicely; for severe postoperative bleeding, injection of some anesthetic (0.5 mL) in a wing block fashion will act as a volumetric tourniquet (anesthetic tamponade of the nail unit) until clotting occurs. Electrocoagulation should not be used. Subungual hematoma is a rare complication of nail surgery because the nail plate should be laid back over the nail bed/matrix rather than tightly fixed in place.
Nail infections rarely occur after nail surgery because surgery is performed in a sterile environment and digits are well vascularized. Daily wound care further limits postoperative infection. Most infections result from poor homecare and/or lack of hygiene.
Necrosis is an unpredictable complication. It may occur after the accidental extended use of a tourniquet, from the use of lidocaine with epinephrine in patients with impaired
blood supply of the limbs, from overly tight stitches, or from excess volume infiltration of local anesthetic.
Postoperative dysesthesia after nail surgery is common. In one study, a sensory disturbance was observed in about half of all patients, without any relationship to the extent of the surgery undertaken.27 There is no clear explanation for this phenomenon.
Implantation cysts were reported as being the most common complication after fullthickness grafts following complete nail unit excision.28
Complex regional pain syndrome is a poorly understood, idiosyncratic, dreaded, and thankfully very rare complication of nail surgery. Pain is severe, out of proportion to the surgical intervention, and may spread up the limb. Associated signs include textural changes of the skin (atrophic), altered adnexae (altered sweating, loss of hair in affected areas), stiffness, and reduced range of motion of nearby joints. Recovery may be partial or complete and is aided by early intervention in consultation with a neurologist.
CONCLUSIONS
Nail surgery is often a part of the diagnosis and management of nail disorders. Knowledge of nail anatomy and physiology are prerequisites to successful nail surgery. By targeting the source of pathology with the least invasive surgical approach, the surgeon obtains diagnostic material for dermatopathology while limiting the risk of postoperative complications.
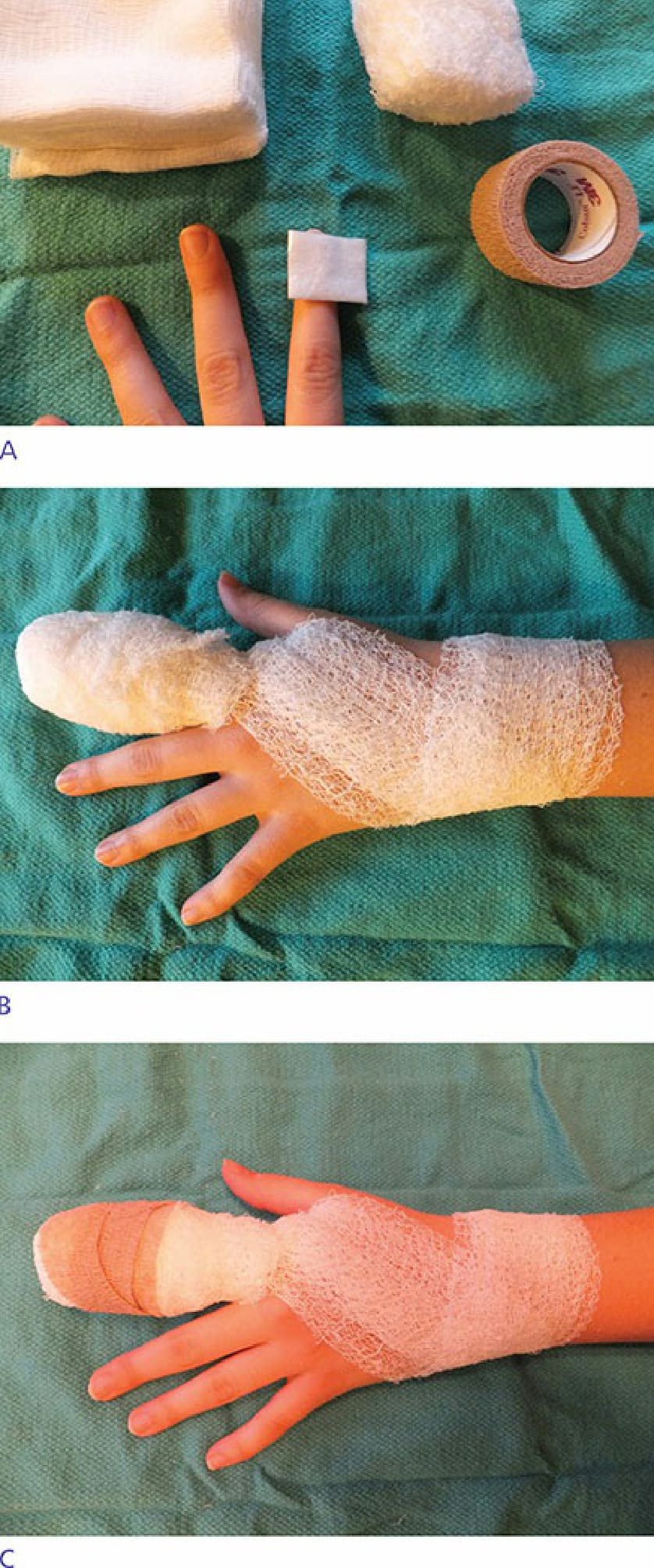
Figure 34-22. (A,B,C) Aggressive bandaging helps maintain immobility.