Nail Bed
Nail Bed
When the source of pathology based on physical examination findings is noted to be in the nail bed, a nail bed biopsy is indicated. If an incision is necessary, align it along the longitudinal axis of the digit to limit the risk of scarring and postoperative nail deformities, including split nail.
Punch Biopsy of the Nail Bed. A 3- to 4-mm punch biopsy of the bed will heal via secondary intention with very little risk of scarring (Fig. 34-12A–C).
A common indication for this procedure is the differential diagnosis of subungual hyperkeratosis that may result from nail psoriasis or lichen planus. Squamous cell carcinoma of the bed is also a common indication. The punch tool is inserted to the bone using a twisting motion. A narrow-tipped scissor such as iris scissor is used to snip the base of the specimen off the periosteum. This can be best achieved by inserting the scissor tips perpendicular to the nail bed surface down to periosteum with the curvature facing upwards, then opening the tips and turning the open scissor tips along the base of the biopsy specimen. The biopsy specimen then can be snipped free from the periosteum. If possible, harvest the specimen with the scissors, as using forceps may crush the delicate specimen. Always check that the punch tool is free of tissue prior to discarding.
Nail Bed Incisions. The nail bed is incised to remove a nail bed tumor (e.g., squamous cell carcinoma, onychopapilloma) or to reach a deep tumor (e.g., glomus tumor of the nail bed or subungual exostosis). After a partial or a lateral plate avulsion, the area of the involved nail bed is fully exposed. Any incision on the bed should be aligned along the longitudinal axis of the digit to limit the risk of scarring and postoperative nail deformity.
The elliptical excision is carried with a #15 blade and should be no wider than 4 mm to limit the risks of onycholysis (Fig. 34-13A–D). The nail bed adheres strongly to the bony phalanx, and is therefore relatively immobile. Re-approximation of tissue edges requires wide undermining of the lateral edges of the wound with the blade. Undermining should be carried out at the level of periosteum, skimming the bone. For larger defects, longitudinal releasing incisions parallel to the lateral edge of the ellipse, associated with lateral undermining, are often required. High tension across the sutures is not recommended, as the fragile nail bed may tear off. Part of the defect may be left to heal by secondary intention. Suturing is performed with 5-0 absorbable suture. The plate is always put back in place (though some lateral trimming may be necessary) and secured to the lateral nails folds.
Matrix When the source of pathology is in the nail matrix, then a nail matrix biopsy is indicated. The main indication for matrix biopsy is longitudinal melanonychia. This should be performed as an excisional biopsy to ensure complete examination of the pigmented lesion by the pathologist. Complete visualization of the matrix area is mandatory. This is perfectly achieved with a proximal partial nail avulsion completed with a reclination of the proximal fold.
In some cases, the matrix is incised to reach a submatricial tumor. Incisions on the matrix should preferably be aligned along the transverse axis of the digit to limit postoperative nail deformity, especially split nail.
The origin of pigmented streaks causing longitudinal melanonychia can be localized by dermoscopy of the free margin of the nail plate (Fig. 34-14).17 As the distal nail matrix gives rise to the undersurface of the nail plate, biopsies in this area have a low risk of scarring. Because the proximal nail matrix gives rise to the upper part of the nail plate, biopsies in this area are more likely to induce surface dystrophy or nail scarring.
Punch Biopsy. This procedure is a very simple and easy option for pigmented lesions of the distal matrix less than 3 mm in diameter.18 After a proximal nail avulsion exposing the entire matrix, the pigmented macule is removed with a punch technique down to the periosteum and harvested in the same fashion as described for nail bed punch biopsies (Fig. 34-15A–D). The plate is replaced and secured to the lateral nail fold (Fig. 34-15E).
Tangential Shave Biopsy. Tangential shave biopsy of the matrix is an extremely useful technique and is widely regarded by many nail surgeons as the preferred method for removal of wide (>4 mm) macular pigmented lesions of the matrix, including the proximal matrix.18 This technique, while technically demanding, provides outstanding results in skilled hands, and allows adequate diagnosis in all cases. Its main drawback is a recurrence of the pigmentation in about 75% of cases.19 Removal of a thin layer of matrix may result in a thinner nail, and very rarely, nail dystrophy.
After partial nail avulsion to expose the matrix, a shallow incision is carried out around the pigmented zone, with extra margins. The scalpel is then held horizontally, and the lesion is removed from the deep dermis using a gentle sawing motion. The specimen should not be thicker than 0.5 mm. The specimen is placed, properly oriented, on a nail template in a cassette for the pathologist (Fig. 34-16). The avulsed nail is replaced and secured to the lateral fold.19
Lateral Longitudinal Excision (En Bloc Excision). For laterally located longitudinal melanonychia or other tumors (e.g. squamous cell carcinoma in situ), lateral longitudinal excisions are indicated.18 The patient must be informed that this type of biopsy will narrow the nail permanently due to partial amputation of the lateral horn of the matrix.
The specimen should not exceed 3 mm in width in order to avoid postoperative lateral deviation.20 The incision begins halfway between the cuticle and the crease of the distal interphalangeal joint and runs distally through the proximal nail fold, and the nail plate/nail bed, until the hyponychium is reached. A second incision performed in the lateral nail fold parallels the first, and joins it at the tip of the finger. Proximally, the incision takes on a laterally curved direction that extends about 5 mm laterally in order
to remove the lateral horn of the matrix (Fig. 34-17A).20 This is especially important when biopsying the great toenail. The specimen is then carefully detached from the bone with fine scissors. At the proximal tip of the biopsy, the matrix must be preserved, and particular care should be taken to avoid raising the scissors too soon and foreshortening the specimen. The defect is reapproximated with horizontal mattress stitches in order to recreate a lateral nail fold (Fig. 34-17B). This type of excision allows the study of the whole nail apparatus: proximal nail fold, matrix, nail bed, nail plate, and hyponychium. The laboratory and dermatopathologist should be experienced with handling such specimens and section them longitudinally to allow visualization of the architecture of the pigmented lesion.
Matrix Excisions. Sometimes, the pigmented macule may present as a narrow longitudinal patch. This may be removed using a longitudinal ellipse with minimal margins. The edges of the incision are widely undermined and reapproximated with 5-0 or 6-0 absorbable sutures. The nail is laid back in place and sutured to the lateral nail fold. If the proximal nail matrix is not involved, the risk of dystrophic sequelae is very unlikely. Another removal option is the tangential excision.
Other indications for matrix excisions are submatricial tumors, such as a glomus tumor, superficial acral fibromyxoma, or pseudomyxoid cyst. Incisions are carried out in transverse or curvilinear fashion with a #15 blade in the distal matrix, a few millimeters behind the junction of the nail matrix and nail bed. Closure with 5-0 or 6-0 absorbable suture should be performed delicately under minimal tension (Fig. 34-18A– G).
Flaps Two central flaps are used in nail surgery. The first is a combination of two small longitudinal bridge flaps, used to close a defect larger than 5 mm on the nail bed (Fig. 34-19A–C). This approach limits the possibility of residual onycholysis. Two longitudinal strips of nail bed, each about 4 mm wide, are freed from the bony phalanx by careful undermining, leaving their proximal and distal attachments in place. These two bridge flaps are mobilized toward the center and reapproximated in the midline with 5-0 absorbable sutures. This is covered by the plate which is secured to the lateral folds.
The second most common flap is a bridge flap used to close a wide lateral defect (usually 1/3 to 1/2 of the lateral nail unit) on the bed (Fig. 34-20A–E). This occurs most
frequently after Mohs surgery for squamous cell carcinoma. This bridge flap comes from the lowest part of the lateral fold and from the pulp. It is elevated to perfectly close the defect on the bed, and it is sutured to the lateral aspect of the plate. The defect on the pulp is allowed to heal by secondary intention.
Grafts Grafting is required after en block resection of the nail unit either from a squamous cell carcinoma or from melanoma in situ, as amputation is not mandatory in these instances

Figure 34-12. (A,B,C) Nail bed punch biopsy.
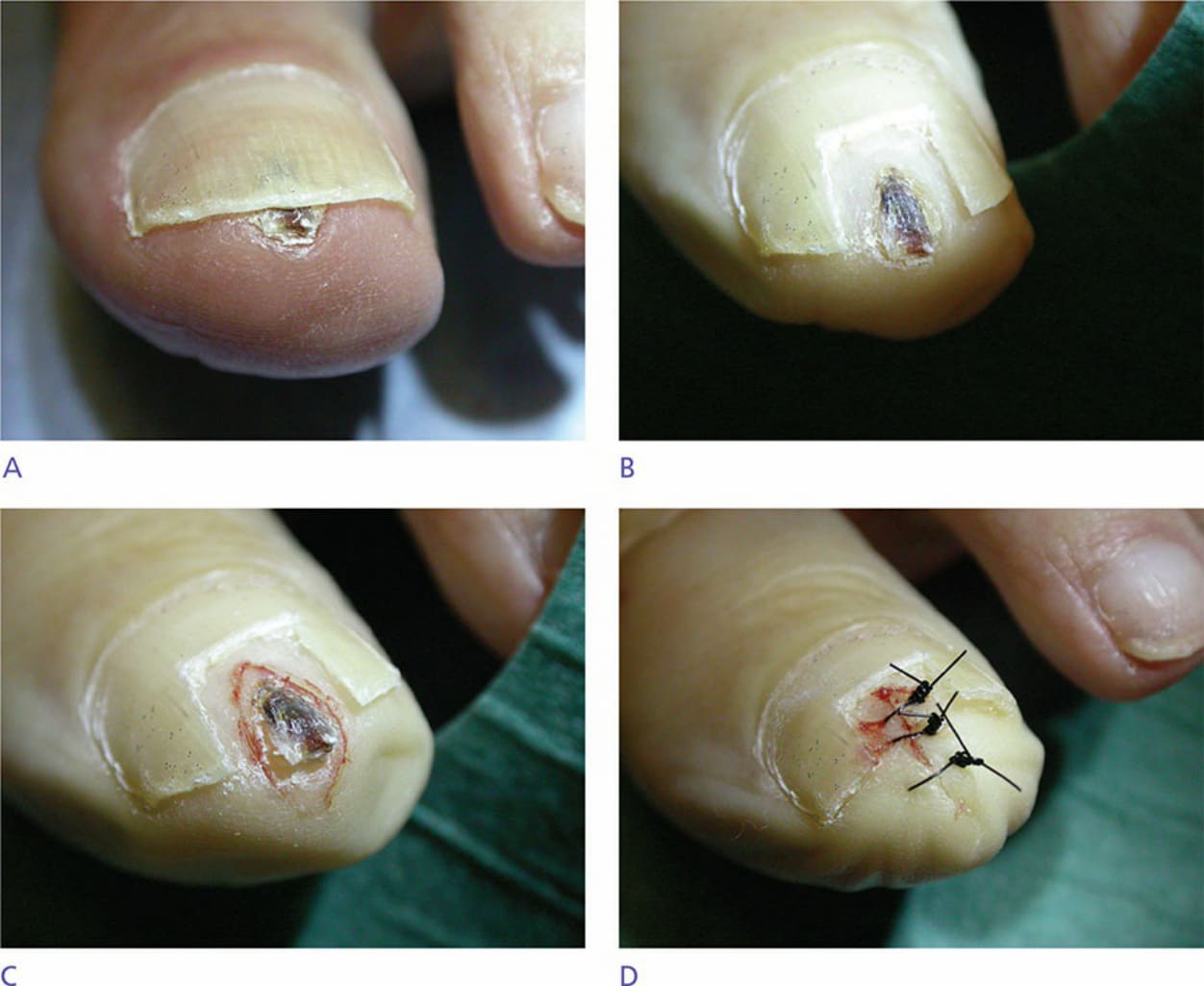
Figure 34-13. Excision of nail bed. (A) Onychoclavus of distal nail bed. (B) Nail plate removal to expose onychoclavus. (C) Appearance of nail bed after excision of onychoclavus. (D) Sutured defect after excision of onychoclavus.
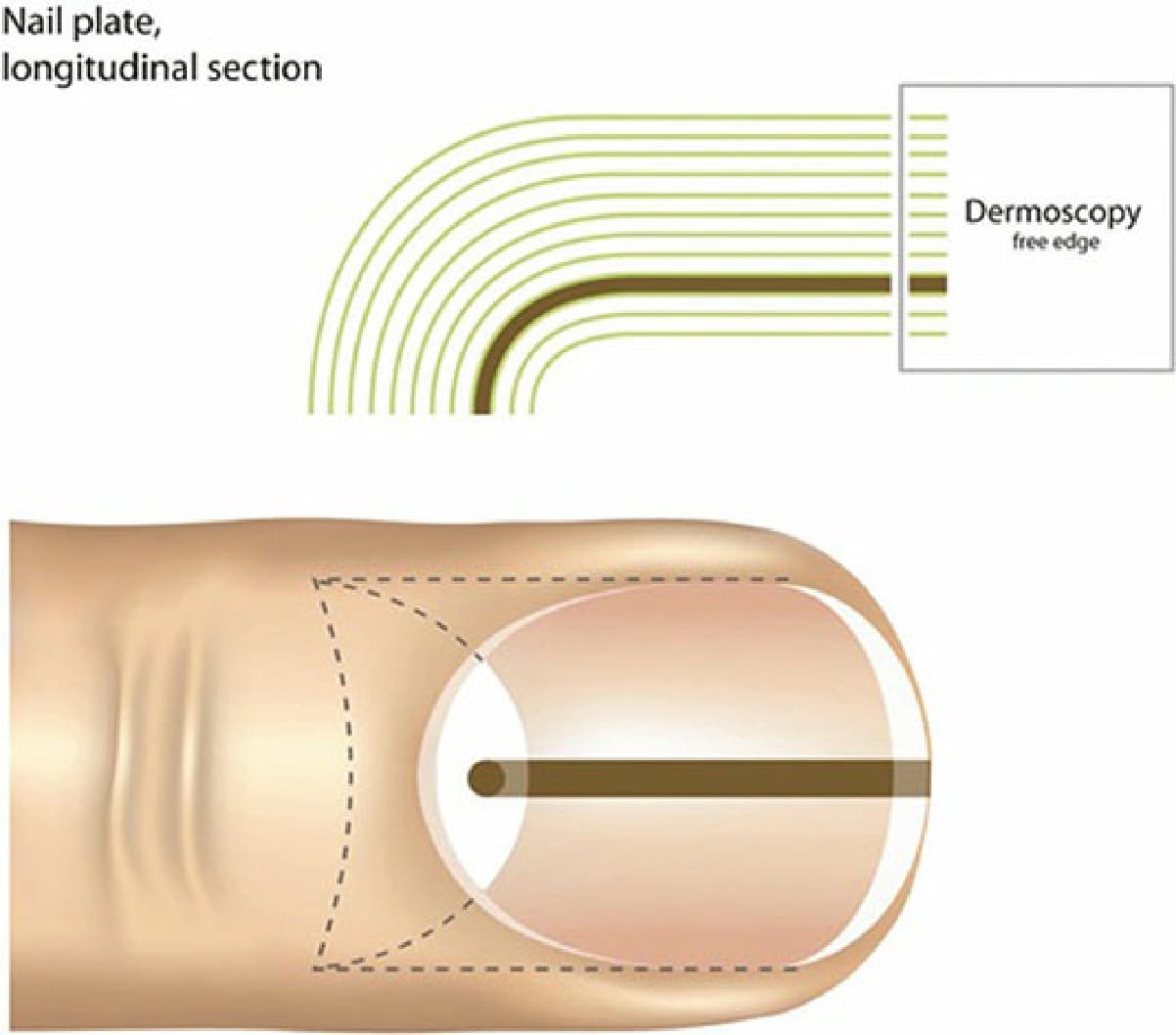
Figure 34-14. Diagram of origin of pigment. The origin of melanonychia can be localized by dermoscopy of the free margin of the nail plate.
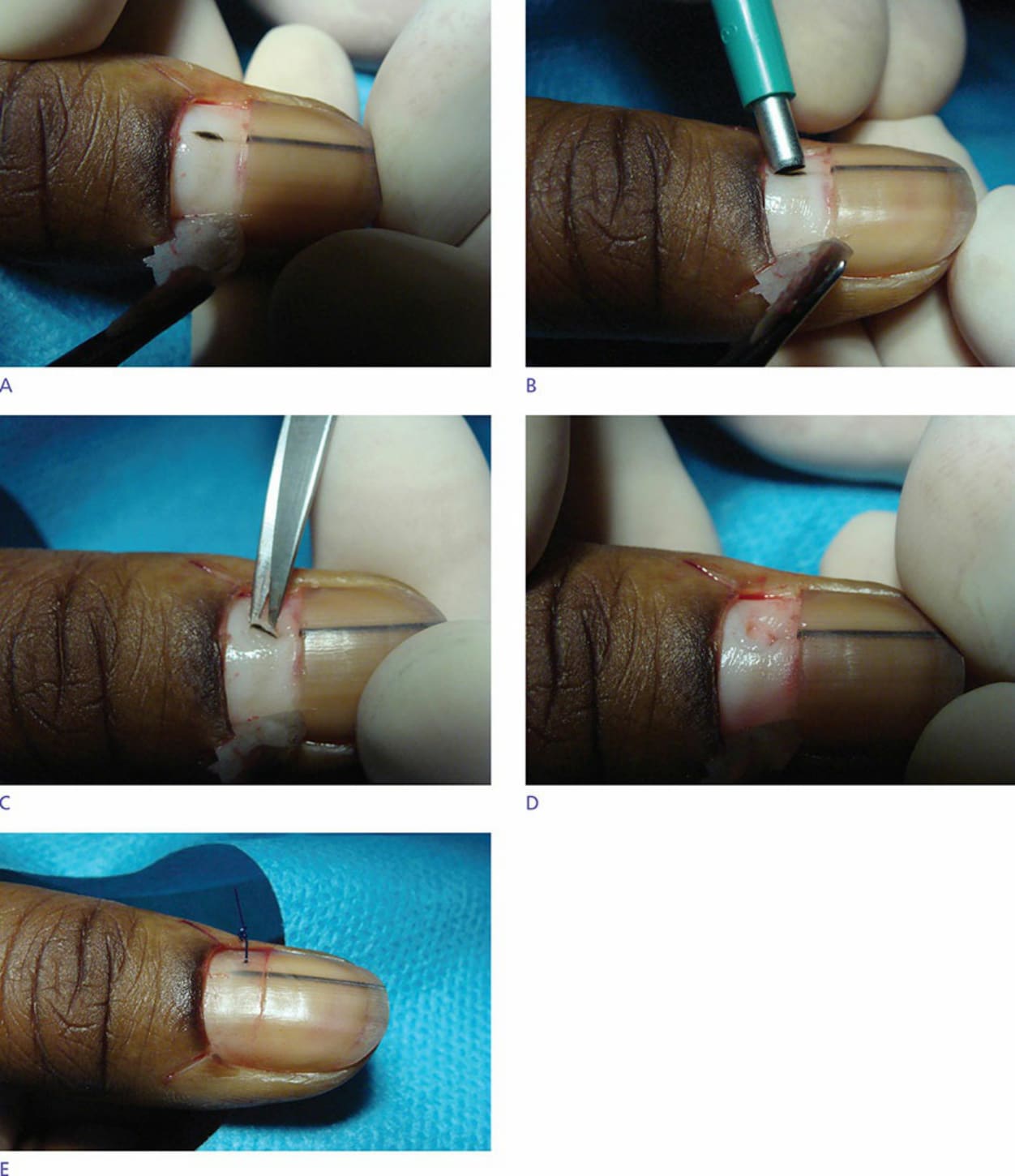
Figure 34-15. (A) Proximal avulsion exposes matrix and pigmented macule. (B) Punching the macule. (C) Harvesting the specimen with scissors. (D) Defect in the matrix left for secondary intention healing. (E) Nail plate replaced and sutured to the lateral nail fold.
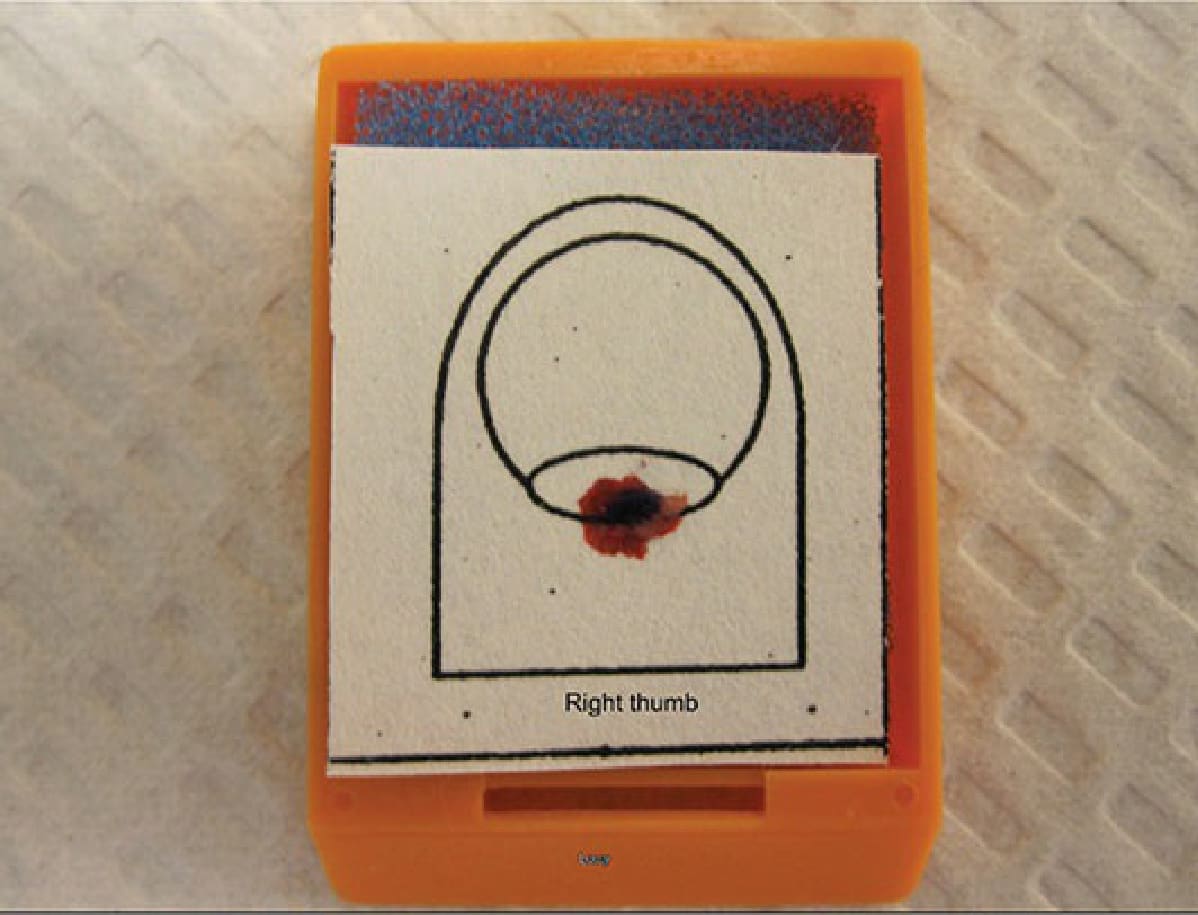
Figure 34-16. Nail specimen submission. Filter paper keeps the specimens flat and immersed in formalin during fixation. Depicted is a specimen resultant from tangential shave biopsy of a pigmented lesion of the nail matrix that was confirmed to be a benign junctional nevus.
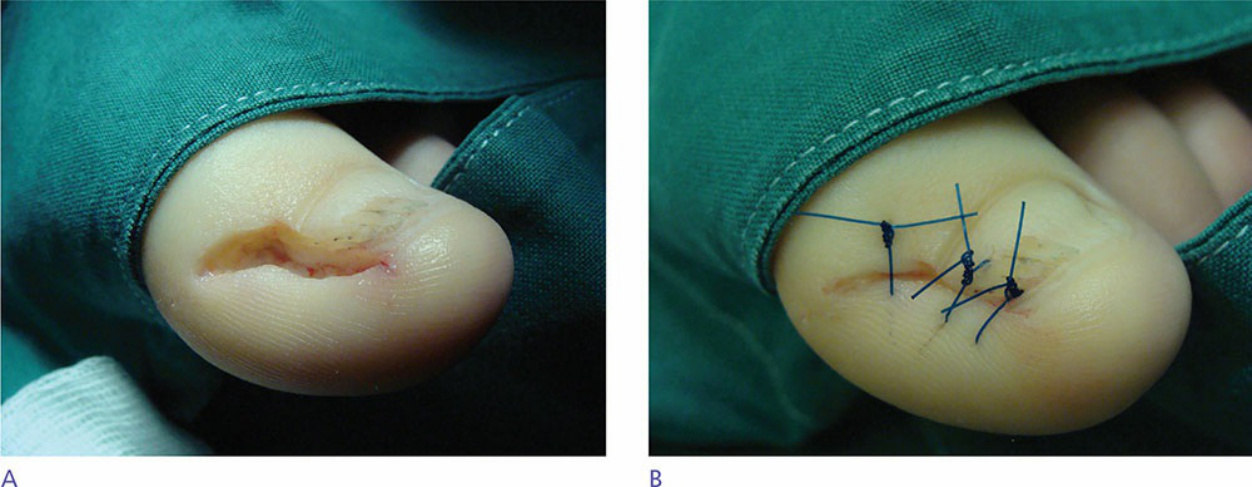
Figure 34-17. (A) Lateral longitudinal biopsy: utilized for diagnosis of lichen planus in a child. Note the lazy S incision that curves proximally to be sure to remove the lateral horn of the matrix. (B) Lateral longitudinal biopsy: suturing perfectly reapproximates the edges of the excision.
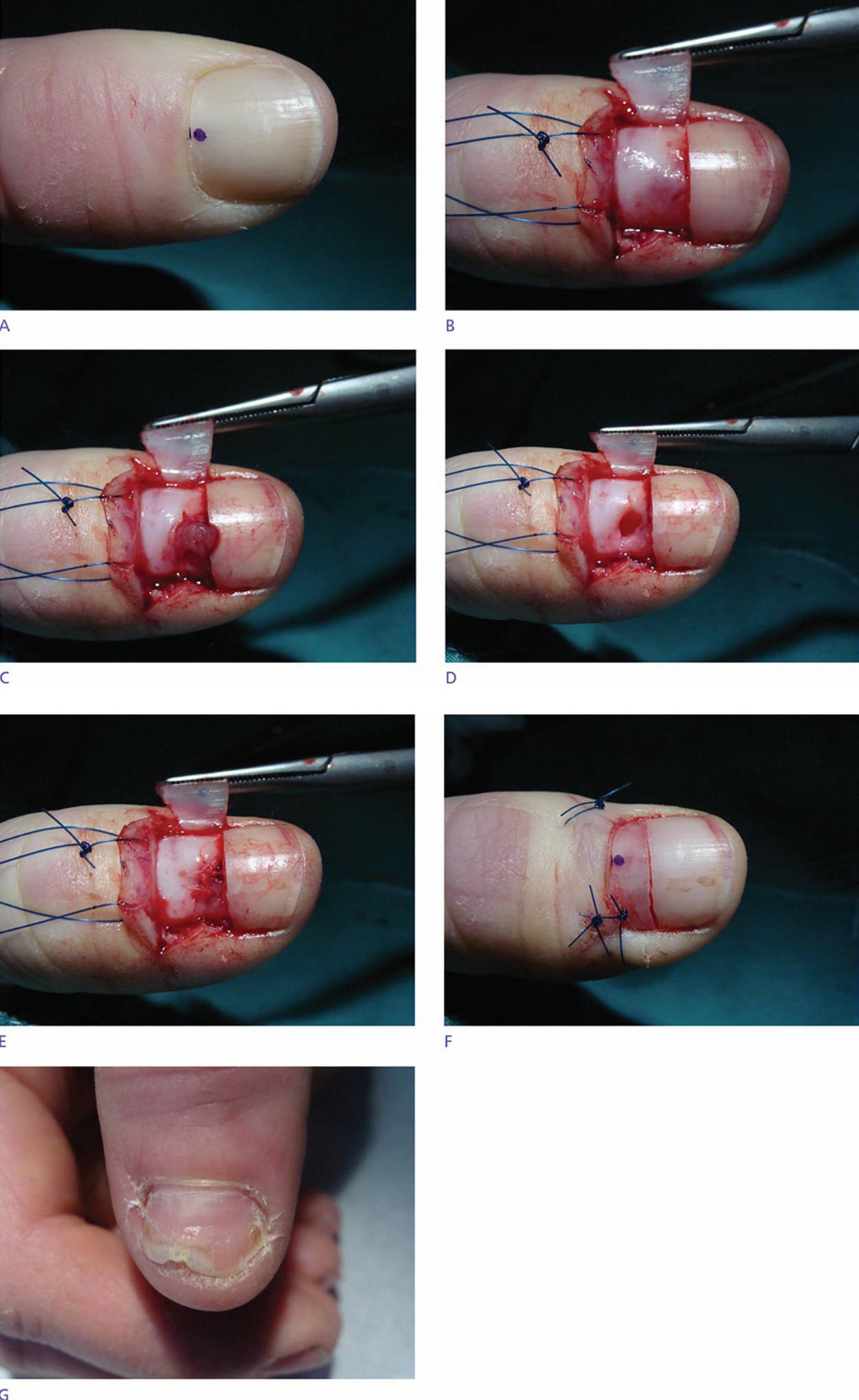
Figure 34-18. (A) Glomus tumor distal matrix. Provoked by Love test. (B) Proximal avulsion exposing matrix. (C) Incision of the matrix and extirpation of the tumor. (D) Defect after tumor removal. (E) Appearance after suturing the matrix. (F) Replacing the plate and securing to nail folds. (G) Appearance at 4 months postoperatively. Nail regrowing without dystrophy.
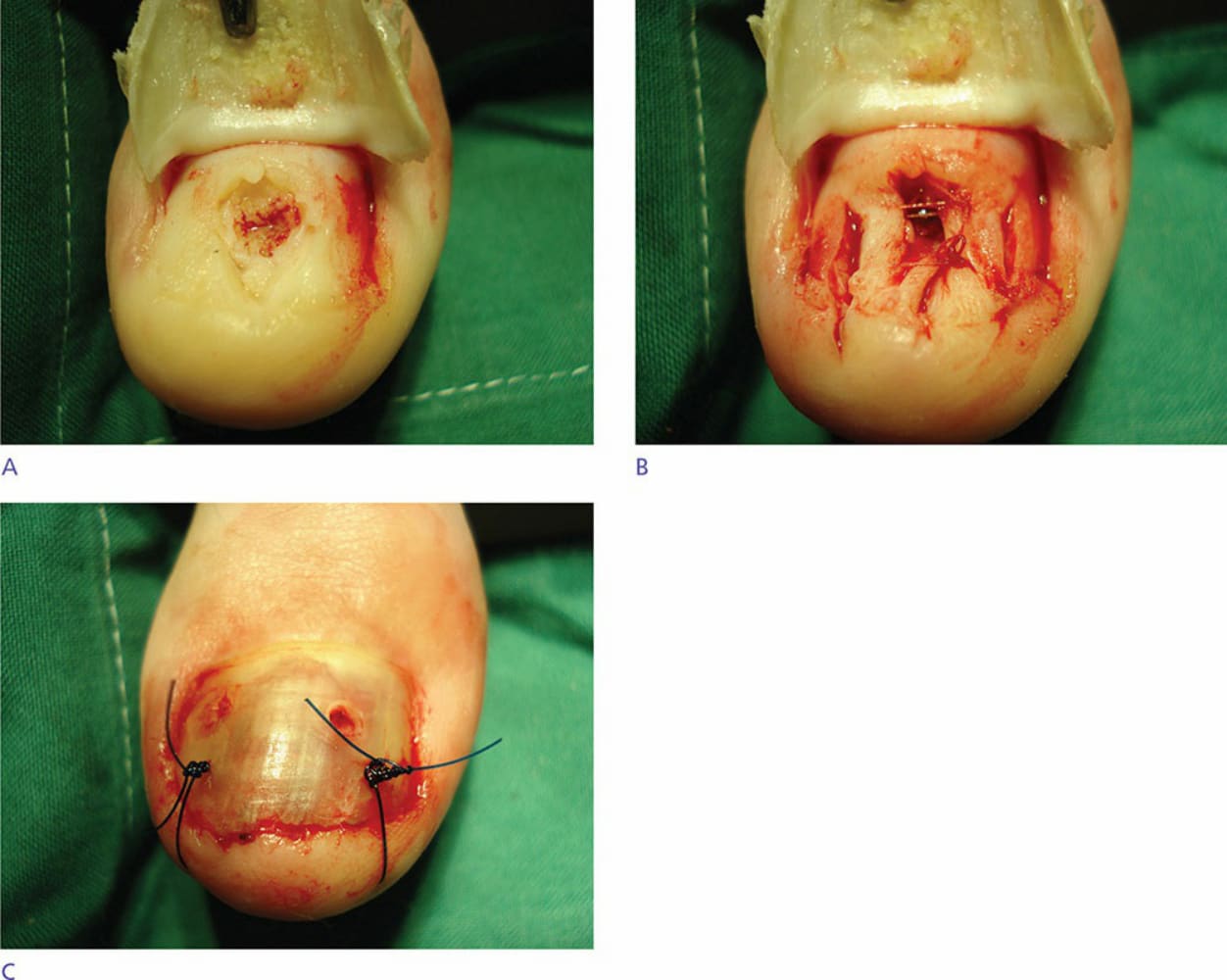
Figure 34-19. (A) Nail bed excision with flap repair. Defect after removal of exostosis. (B) Flap repair. Reduction of the size of the defect by two small lateral bridge flaps. (C) Appearance immediately postoperatively. Nail plate put back in place and secured to distal fold. Two punches in the plate allow drainage of oozing.

Figure 34-20. (A) Approach to the bridge flap, used to close wide lateral defects (here due to squamous cell carcinoma in situ of the lateral nail unit). (B) Appearance after clear margins were obtained using Mohs micrographic surgery. (C) Closure with a bridge flap from the pulp. (D) Appearance at 8 months postoperatively. (E) Upper view showing the permanent narrowing of the nail unit.
(Fig. 34-21A–C).21,22
(Fig. 34-21A–C).21,22
Grafting should generally only be considered on fingers. Retaining some underlying soft tissue in the graft is a must, as cicatricial tissue adhering to the bony phalanx may be very uncomfortable when using fingers for a manual task. The graft is usually harvested from the ipsilateral arm, in a nonhair-bearing area, such as the internal aspect of the upper arm. Defatting should not be overly aggressive in order to maintain some padding. On the toes, secondary intention healing is best, as background edema, as well as direct pressure from shoes and from possible seroma formation almost always leads to necrosis, and toe cosmesis is generally of less concern.
Nail Bed Reconstruction Late reconstruction of the nail bed often heals with scarring and dystrophy.23 Wounds less than 5 mm in their broadest dimension can be left to heal by secondary intention, but may still result in scarring and nail deformity. Defects measuring 3 to 5 mm can be closed with lateral advancement flaps, mobilized toward the center by the use of relaxing incisions in the lateral paronychial folds (see above).
Defects greater than 5 mm can be treated with a split-thickness nail bed graft harvested from a less visible digit.4 A split- or full-thickness nail bed graft up to 10 mm in diameter will typically survive even when placed directly onto the bony phalanx.24 The main drawback of such techniques is that they often induce a new defect on another nail. To overcome this inconvenience, some surgeons harvest mucous membrane from the hard palate and graft it onto the nail bed with good results.25
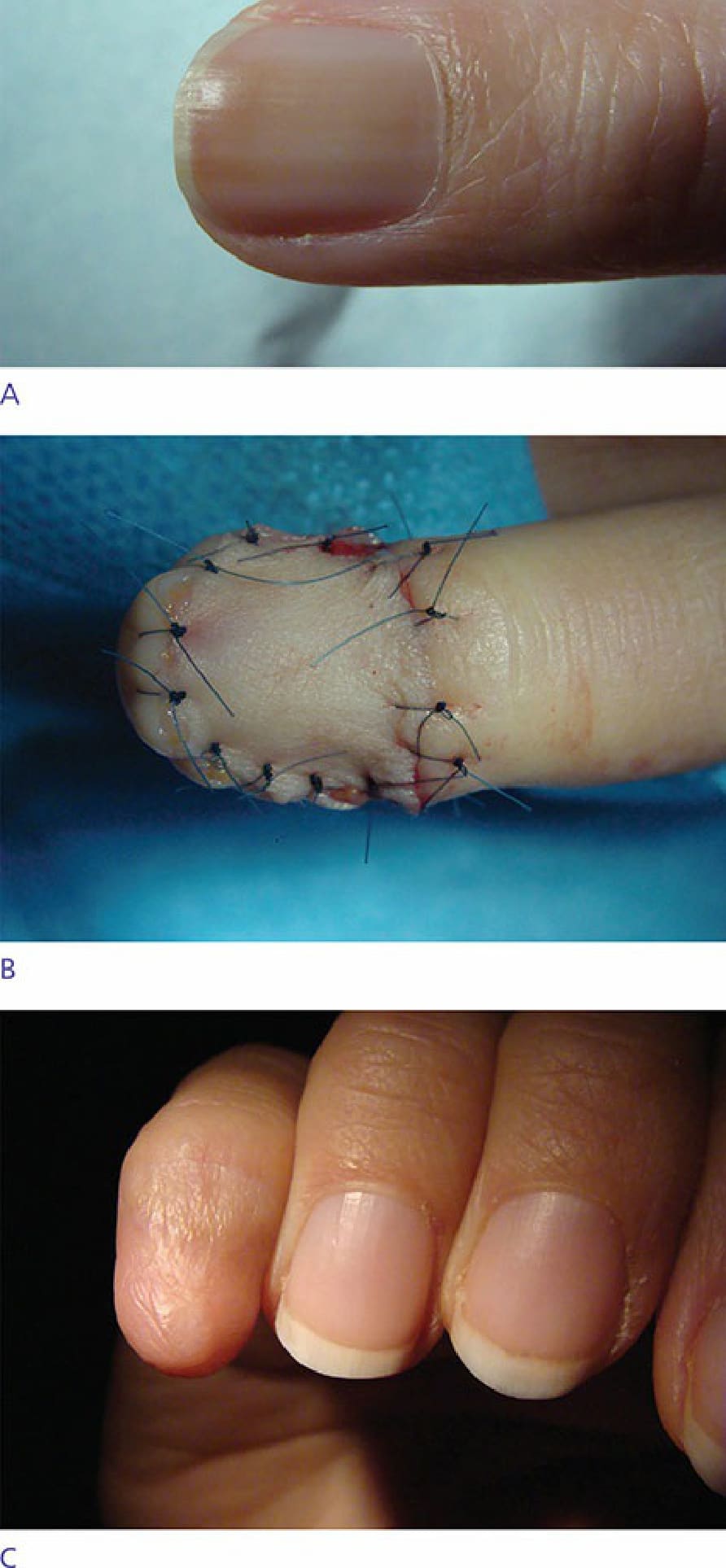
Figure 34-21. (A) Full-thickness skin graft for repair of excision of melanoma in situ. Melanoma in situ of the second finger. (B) Appearance immediately postoperatively after placement of a full-thickness skin graft. (C) Clinical appearance of second digit at 1-year follow-up after the placement of full-thickness skin graft.