Avulsion
Avulsion
Depending on the source of nail pathology, avulsion of the nail plate may be necessary for adequate visualization. When possible, a partial nail avulsion is preferred to complete nail avulsion. Partial nail avulsions may, for example, be distal, proximal, lateral, or “trap-door” (Fig. 34-10).12,13
The most common approach is the distal one: an elevator is gently slid under the proximal fold in an anterior–posterior motion until it is completely freed from the nail plate. The elevator is then advanced under the nail plate until resistance is lost,
signifying that the matrix, with its loose attachment to the nail plate, has been reached. This anterior–posterior movement is repeated several times from one side of the nail plate to the other to avoid injuring the fragile longitudinal nail bed ridges. Caution must be taken to detach the lateral horns of the nail plate fully by firmly pushing the instrument in posterolateral angles. Then, one lateral portion of the nail plate is grasped with a hemostat, and the nail plate is avulsed with an upward rotating motion, as would be used to open a sardine can.6 The opposite lateral side of the plate is left attached. This procedure exposes the entire nail bed area as well as the distal matrix. Avulsion of the proximal third of the nail plate, combined with reclination of the proximal fold, exposes the complete nail matrix area (Fig. 34-10B). Another option is the “trap-door avulsion,” where the plate, once fully detached from its bed, is lifted up as the hood of a car (Fig. 34-10D).12
Replacing the partially avulsed nail plate after surgery reduces postoperative pain. The nail plate serves as a biologic dressing promoting healing and protecting the more delicate underlying structures. The nail should be secured to the nail unit with 5-0 nonabsorbable nylon. To accomplish this, first, drill a 1-mm hole through the nail plate using an #11 blade. Next, pass the suture needle though the soft tissues and then pass the needle through the predrilled hole. There are, of course, instances in which the nail plate cannot be replaced because it is too dystrophic or it must be submitted for microscopic and/or microbiologic evaluation.
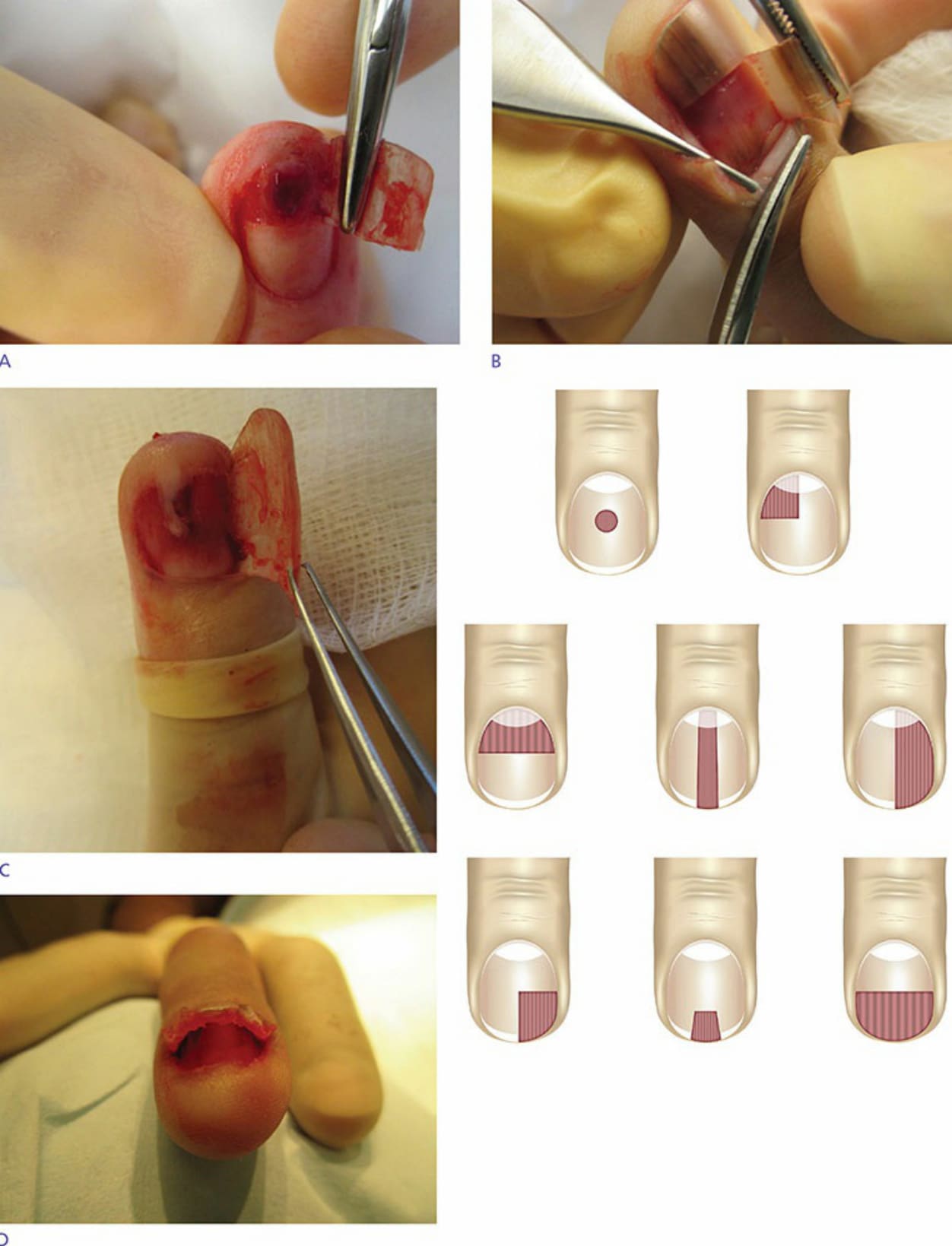
Figure 34-10. (A) Distal partial avulsion. (B) Proximal partial avulsion. (C) Lateral longitudinal partial avulsion. (D) Trap door avulsion. In each instance, the nail plate is freed with a freer elevator, cut transversely with an English anvil nail splitter, and rolled laterally, then replaced after the surgical specimen is harvested. (E) A wide variety of partial avulsion patterns are possible.