Debulking
Debulking
Many surgeons curette the lesion until visually normal skin is reached to help identify the tumor margins.26,27 To perform curettage, a curette is scraped over the tumor in different directions with moderate pressure, producing fragments of friable tumor that can be wiped away to reveal a clean wound base or to produce a vertically oriented slide of tumor pathology when a previous biopsy is unavailable or has not been done (Fig. 29-4). Curettage is helpful in debulking friable tumor prior to MMS, but it does
not reliably delineate the entire extent of a tumor.27,28 Infection, crusting, hyperkeratosis, background seborrheic dermatitis, and actinic keratoses may exaggerate the tumor size, resulting in an overly large debulking layer.
Since most MMS occurs after a diagnostic biopsy, there is frequently an area of eschar overlying the cancer site. Since it is of no clinical value and can interfere with the production of high-quality slides, the eschar should be removed by the surgeon or technician prior to processing the tissue.
Aggressive curettage is not advocated. Curettage may cause shearing forces on the remaining, adjacent epidermis that will be included in the Mohs layer, which may lead to epidermal separation that will appear as clefting at the dermal–epidermal junction or as epidermal loss. In addition, the technician may interpret torn epidermis as a purposeful nick, leading to inaccurate sectioning. In severely photodamaged skin, this can also result in overhanging pieces of epidermis at the edges that can lead to false positives if this free epidermis is embedded near the margin (Fig. 29-5). Floaters are also more common after curettage,29 so care must be taken to wipe the debulked tissue prior to excising the layer (Fig. 29-6).

Figure 29-4. Curettage prior to taking of first Mohs layer to debulk the tumor and clinically assess the gross tumor margins.
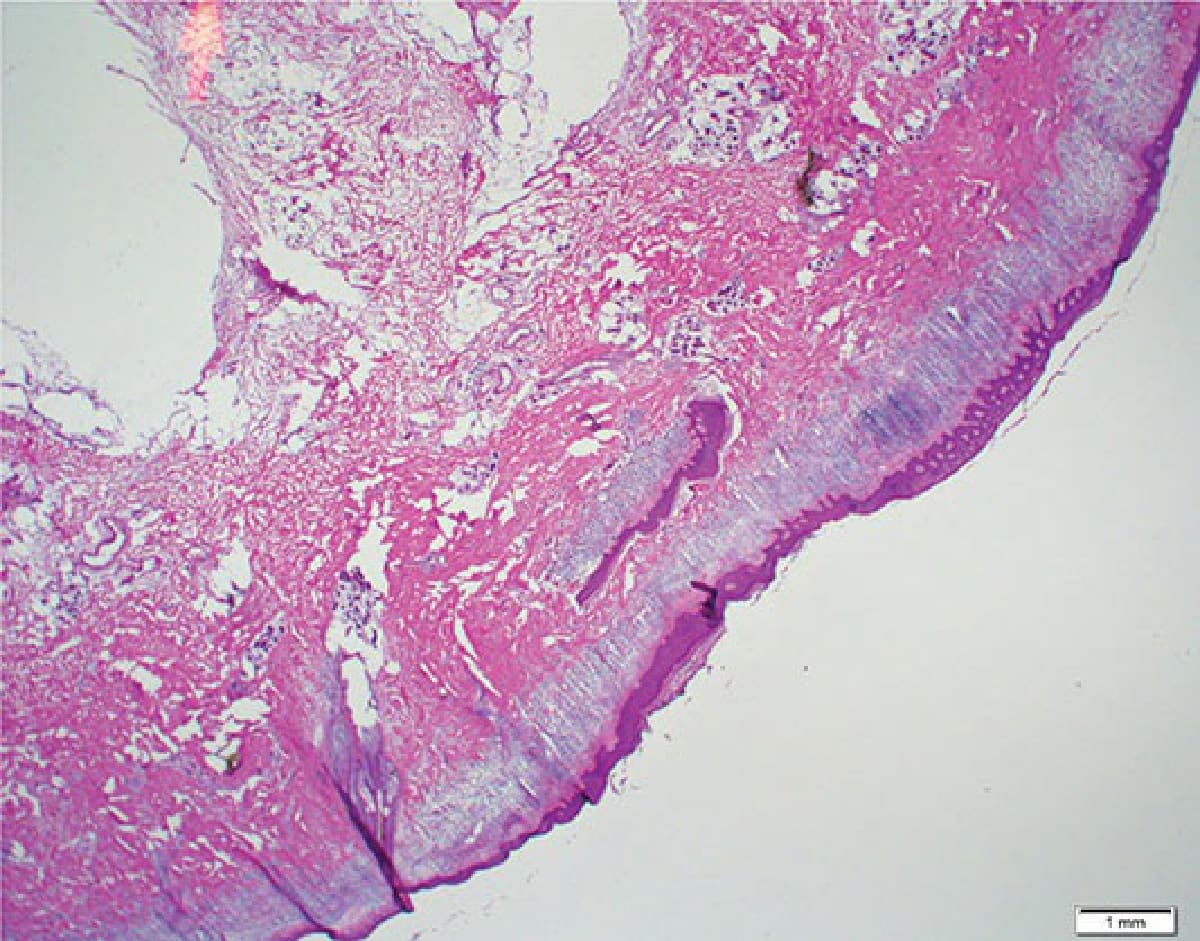
Figure 29-5. An artifact of aggressive curettage with overhanging epidermis implanted into the margin.

Figure 29-6. The curetted tumor is wiped away.