TECHNIQUE
TECHNIQUE
The fundamental technique was pioneered by Frederic Mohs in the 1930s, and his landmark article on 440 patients treated with chemosurgery was published in 1941.23 At that time, Mohs used zinc chloride paste for in vivo fixation prior to surgical removal. Dr. Mohs applied zinc chloride paste to the cancerous skin to fix the tissue prior to excision. The following day, the tissue was excised and examined under the microscope. The process was repeated daily until the tumor margins were clear.
The original in vivo chemosurgical approach transitioned to the fresh frozen tissue technique beginning in 1953, an innovation pioneered by Dr. Mohs for eyelid cancers to prevent ocular damage by the zinc chloride paste. Subsequently, the technique was popularized and described in detail by Tromovich and Stegman in 1974.24 The fresh frozen technique obviated the need for escharotic zinc chloride paste, allowed complete
tumor clearance in 1 day and immediate surgical reconstruction.
The Mohs procedure is considered a clean procedure rather than a sterile procedure. Once the biopsy site is identified with confidence, and patient consent is obtained, the area is typically prepped with chlorhexidine or Betadine and then draped. Local anesthesia is first infiltrated. Lidocaine 1% to 2% with epinephrine 1:100,000 is used most commonly, although nerve blocks and long-lasting anesthetic such as bupivicaine may be helpful to prolong anesthesia (see Chapter 12).
With Mohs surgery, the tumor is removed in a saucer-shaped section and divided into pieces for processing (Fig. 29-2). Evaluation of all excised margins reveals skin cancer present at one edge. The area is subsequently mapped and excised on layer II. With the Mohs method, no tumor is missed. In contrast, bread-loafing of the elliptical excision specimen for histologic examination could miss tumor extending to the margin because only a small portion of the margin is examined.
Appropriate instruments, organization, and setup are essential for optimizing outcomes (Fig. 29-3). The fresh tissue technique of MMS has been simplified into debulking the tumor followed by excising and orienting; sectioning and inking; flattening, embedding, and freezing; cutting and staining; and mapping the tissue. It takes great skill to take a Mohs layer that can be processed perfectly by the lab, and Mohs surgeons should be aware of the technical challenges inherent in each step of specimen processing. The success of the procedure is tied to the precise application of each step of the technique and the expertise of the individuals performing them. Technical errors impact slide quality, and represent the most common cause of local recurrence after MMS.25
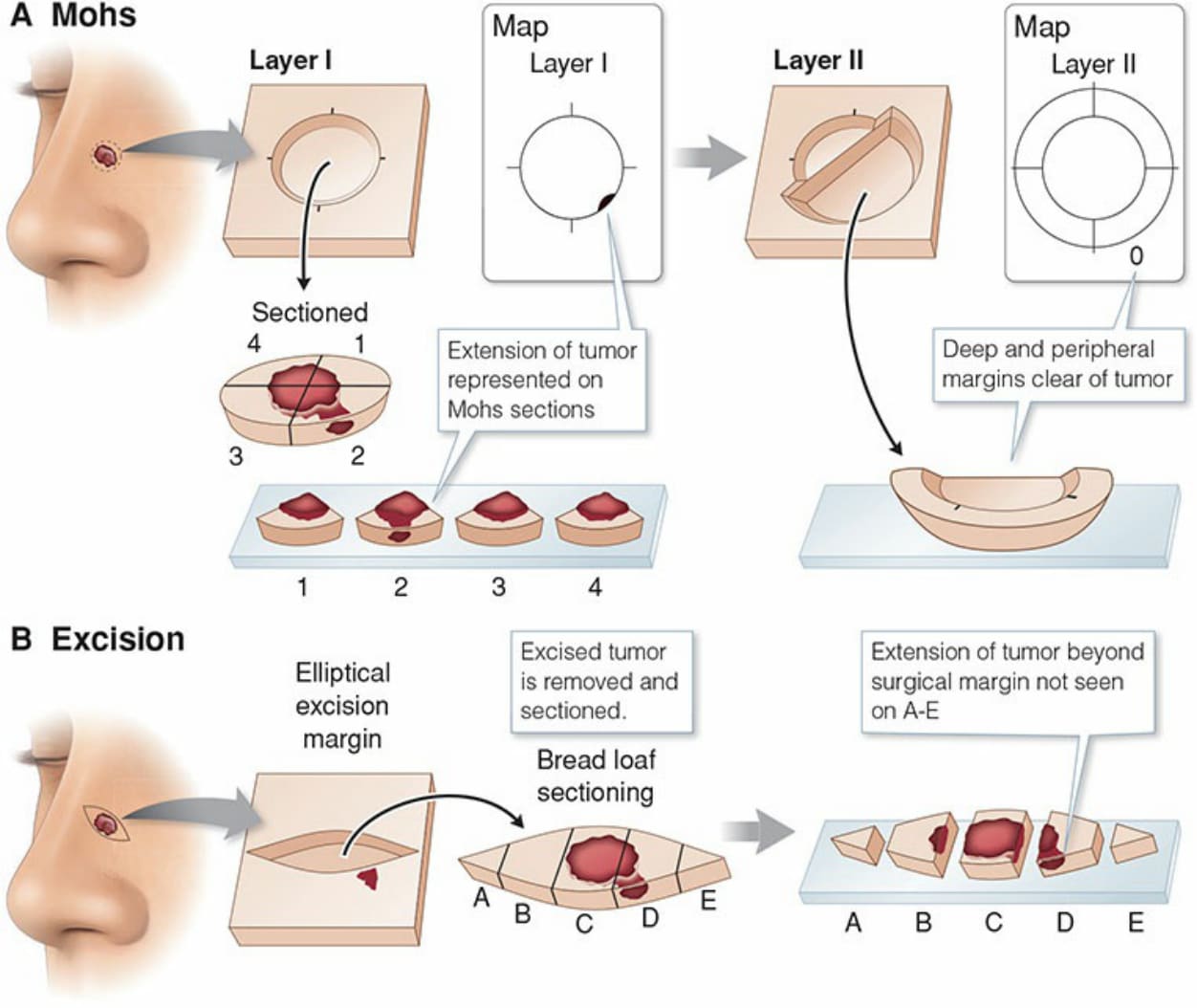
Figure 29-2. With Mohs surgery, the tumor is removed in a saucer-shaped section and divided into pieces for processing. Evaluation of all excised margins reveals skin cancer present at one edge. The area is subsequently mapped and excised on layer II. With the Mohs method of tissue processing, no tumor is missed. In contrast, breadloafing of the elliptical excision specimen for histologic examination could potentially miss tumor extending to the margin since only a small portion of the margin is examined.

Figure 29-3. Standard instruments for Mohs surgery. Clockwise from top left corner: cotton-tipped applicators, blade remover, dental rolls, curved hemostat, forcep, supercut scissors, scalpel with 15 blade, curette, electrosurgery device, gloves overlying towels for draping, towel clamps, gauze, and a ruler.