POSTOPERATIVE CARE
POSTOPERATIVE CARE
Patient education regarding the expected postoperative course and proper postoperative care is imperative for optimal surgical outcomes. The patient should be counseled about normal physiologic color changes seen in a graft during the immediate postoperative period. The graft will initially appear blanched and white. As imbibition begins to take place in the days following surgery, the graft will become edematous and violaceous. As inosculation and neovascularization are initiated and established around 1 week postoperatively, the graft will appear more pink in color. In the months following
surgery, the edema of the graft will dissipate, and the color of the graft will return to the initial color of the donor skin.
The most important pearl in the immediate postoperative care of skin grafts is the avoidance of any shearing forces which will disrupt the inosculation and neovascularization of the immature graft and significantly increase the risk of necrosis. The use of bolster dressings has been advocated to decrease shearing forces and it is some dermatologic surgeons’ preference to routinely employ these. However, the use of bolster dressings has not been definitively demonstrated to increase the chances of graft survival.17,18,26 Table 28-2 is a list of pearls regarding the use of grafts and Table 28-3 is a list of pitfalls.
If a bolster is not placed, the pressure bandage placed postoperatively should be left for 24 to 48 hours. After removal, the patient is instructed to gently wash the area with a mild soap and water once or twice daily. The graft is then covered with petrolatum ointment and a sterile bandage. This is repeated until suture removal, which is performed at 5 to 7 days for grafts on the face, 10 to 12 days for grafts on the scalp, and 12 to 14 days for grafts on the trunk and extremities. If a dry tie-on bolster dressing is placed, most dermatologic surgeons advocate keeping the surgical site dry for 1 week postoperatively until the bolster is removed. If petrolatum-soaked gauze for the bolster dressing is utilized, the patient is generally recommended to gently wash around the bolster dressing daily and apply additional petrolatum ointment on and around the
dressing to preserve the moist environment of the surgical site.
If an eschar is present at suture removal, this does not necessarily indicate complete graft necrosis. It is not uncommon to observe superficial slough that can be gently debrided. Grafts that are thicker or on poorly vascularized wound beds are more prone to this outcome. With continued daily cleansing and petrolatum ointment application, many of these grafts will re-epithelialize with a satisfactory aesthetic result. If complete necrosis does occur, the necrotic graft should be gently debrided, and the wound allowed to heal by second intention before any additional revision surgeries or procedures are planned.
The appearance of grafts tends to significantly improve in the 3 to 4 months following surgery. Most patients will require close follow-up and reassurance during the postoperative period. It is recommended to wait at least 3 months before performing scar revision or refinement procedures.
CONCLUSIONS
Skin grafts are most often utilized when primary closure, flap repair, and second intention healing are not feasible or inappropriate for the repair of a surgical defect. Although the cosmesis of skin graft closures can be inferior to that of wounds closed primarily or by flap closure, skin grafts provide a straightforward one-step procedure for anatomic areas with minimal skin laxity. Excellent aesthetic results and functional outcomes are possible with appropriate graft selection, meticulous surgical technique, and patient compliance. A thorough knowledge of the indications, selection, technique, complications, and postoperative care of FTSGs, STSGs, cartilage grafts, and composite grafts is essential for the practicing dermatologic surgeon.
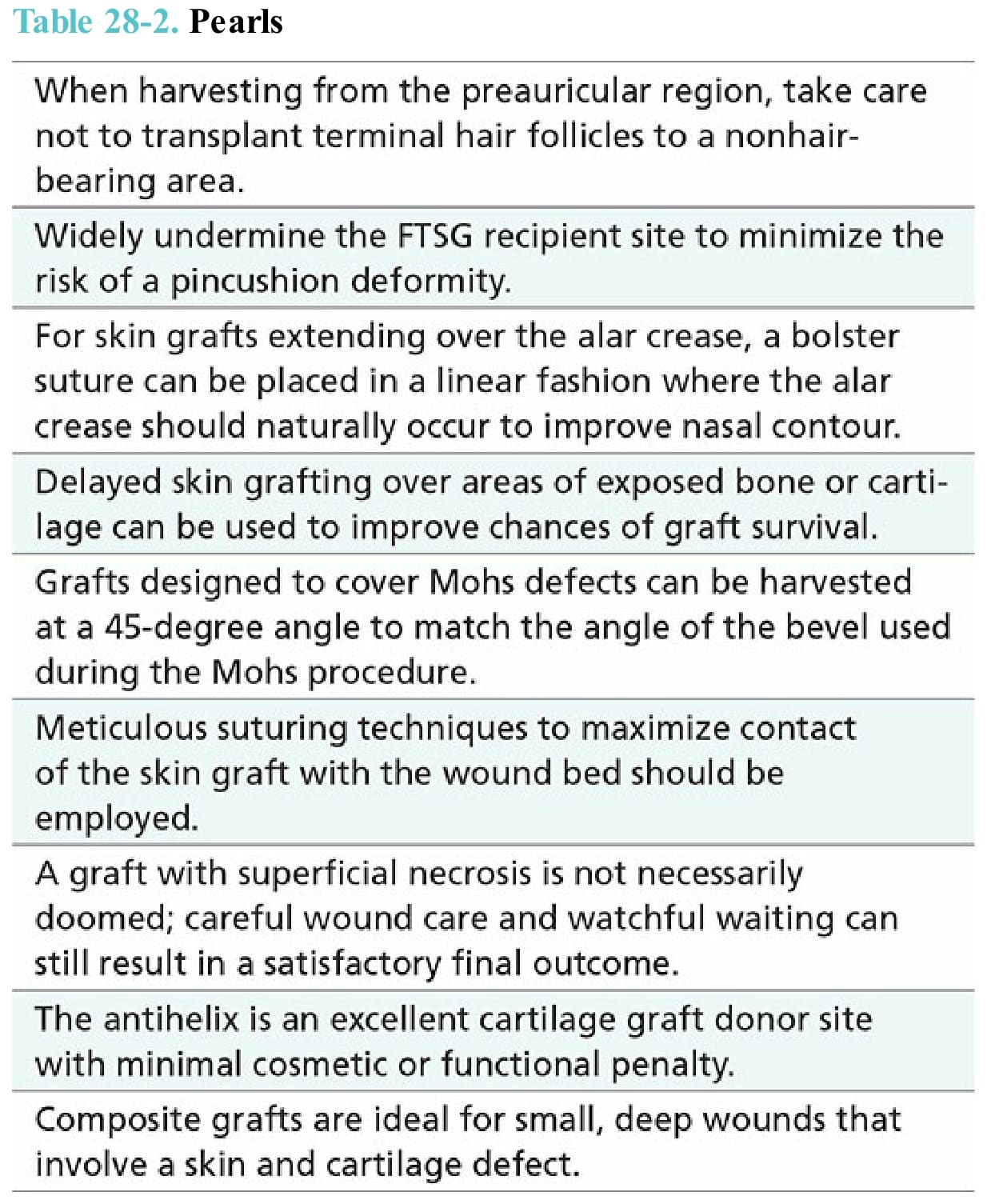
Table 28-2. Pearls
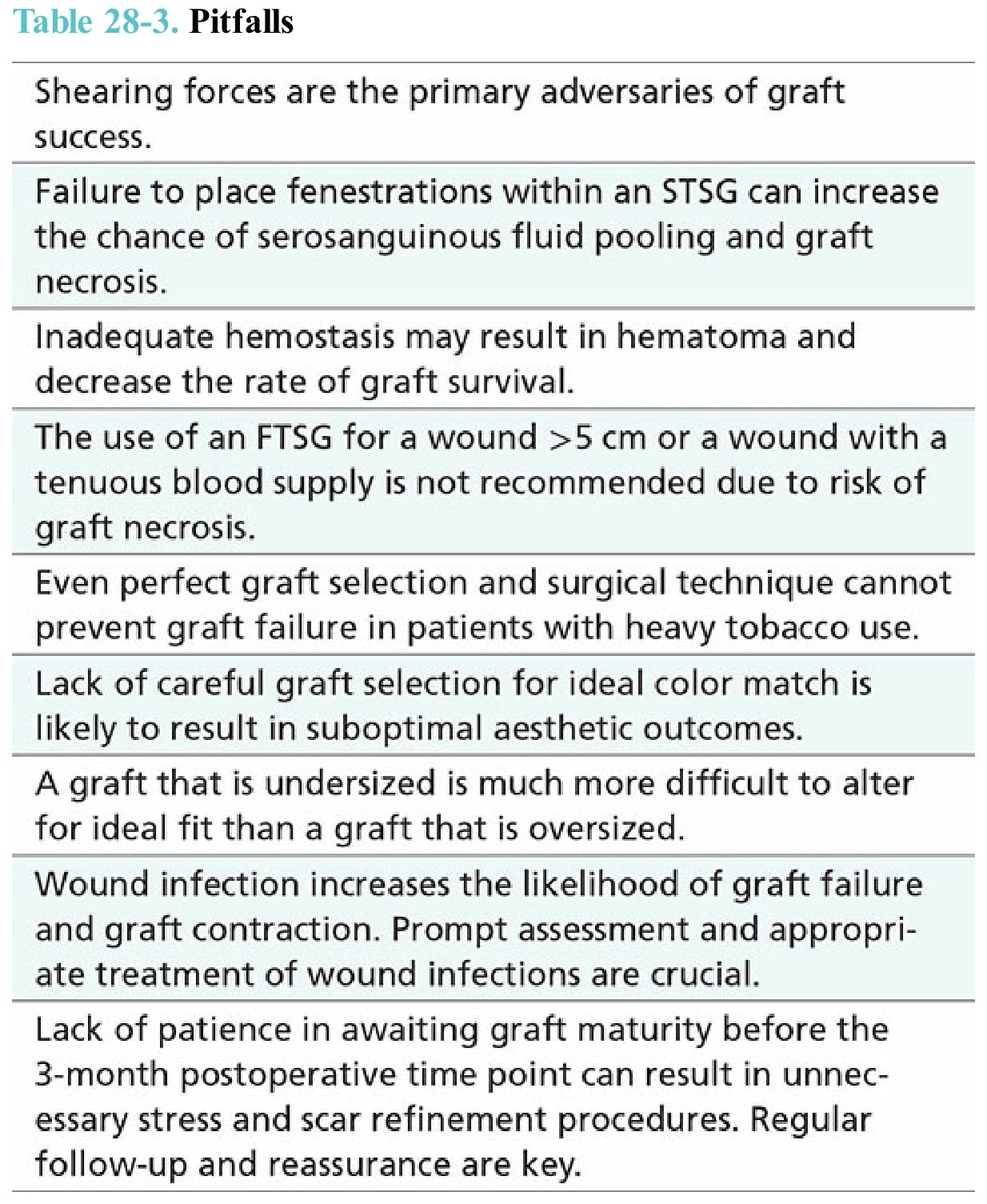
Table 28-3. Pitfalls