Z-plasty variants
Z-plasty variants
Double-opposing Z-plasty includes two mirror image Z-plasty flaps placed immediately adjacent to each another (Fig. 27-3). After transposition of the triangular flaps, which naturally interdigitate with each other, there is a broadly based large flap with a preserved and intact vascular network. This application of the Z-plasty is primarily utilized in the areas of limited skin availability, laxity, or vascularity.19 As such, the technique is most useful in scar contractures, webs, or burns.
The dancing man is a modification of the double- opposing Z-plasty technique (Fig. 27-4). Here, the Z-plasties share a common limb. First described by Mustardé, the dancing man has been primarily utilized in the epicanthal region 20 and later applied to the release of skin contractures.21
The unequal triangle Z-plasty is another variation of the original Z-plasty technique (Fig. 27-5). Unequal triangular flaps are a result of a Z-shaped incision using nonparallel limbs and dissimilar angles between the limb incisions and the central incision. The half-Z is one example of this method, where one of the Z-plasty limbs is perpendicular to the central incision (Fig. 27-5C,D). The unequal angle approach is often utilized when there are different degrees of laxity in regional skin, such as the palpebral area or overlying scar tissue.
The unequal triangle Z-plasty has been adapted in innovative ways. Mutaf et al. designed the “reading man” procedure, a spinoff of the unequal triangle Z-plasty technique for the repair of circular defects of the skin (Fig. 27-6).22 The resultant incisions produce the silhouette of a man who is reading a book held in his hand, and flap transposition results in effective closures for defects up to 14 cm in diameter.22
Consistent findings at mean follow-up of 15 months reveal durable skin coverage with fine scars in all patients.22
The four-flap Z-plasty modestly redesigns the basic Z-plasty to include two extra limbs coming off the end of the central incision, thereby bisecting the original angles (Fig. 27-7). Traditionally, there are two types of four-flap Z-plasty, the 120 and the 90 degrees, with each angle divided in half to create four flaps. One of the greatest advantages of this technique is the considerable decrease in tension and increase in length it provides through the construction and subsequent transposition of four flaps.23 It provides gains of length of two 60-degree Z-plasties (150% increase, at 75% per Zplasty) or two 45-degree Z-plasties (100% increase, at 50% per Z-plasty) performed in parallel.24 Consequently, this technique is often utilized at scar sites of the first interdigital web space of the hand and anterior and lateral neck where contractures often restrict areas of otherwise normal flexion. The four-flap Z-plasty releases these severe scar contractures through the additional length gained.
The four-flap Z-plasty uncovers an important relationship: an increase in the number of transposition flaps yields greater gain in length. This relationship is also applicable to multiple Z-plasties arranged in series (Fig. 27-8). At times, often in the case of long contractures, multiple small Z-plasty in series is superior to the use of one large Zplasty because though the theoretical amount of lengthening in the longitudinal axis along the central limbs are equivalent when comparing both methods, the compound Z-plasty provides less transverse shortening, along the lateral limbs on the horizontal axis and less tension across the common limb.25 Therefore, for long linear scars, the multiple Zplasty is recommended. This procedure aims to divide the central limb into segments which ultimately distribute the tension across various smaller transverse diagonals. The redirection of these forces may improve the appearance of the scar.
Some drawbacks to multiple Z-plasty relate to the degree of tension on adjacent flaps from neighboring transposition flaps. This not only adds to a reduction in the theoretical gain in length, but also leads to flap distortion. Multiple Z-plasty may lead to a sawtooth pattern when applied to a web.26
The traditional Z-plasty technique and associated variations predispose the scar to stereometric elongation, that is, a bulging effects or dog-ear (standing cone) formation, particularly when performing Z-plasty on flat surfaces.27,28 Though normal tensile forces and the elasticity of the skin routinely counter the bulging effect, the outcome is not always flawless, and inelastic skin is most vulnerable to bulging. To circumvent these issues, Roggendorf in 1983 introduced the planimetric Z-plasty which allows for elongation only within the skin plane.28 To achieve this, a Z-plasty with 75-degree angles is created with limb incisions twice the length of the central limb (Fig. 27-9). This central incision is then extended in both directions to create an imaginary diagonal line between the end of the lateral limb incision and the central limb, measuring twice the length of the original limb incisions. The two triangular areas that are created are excised prior to flap transposition. Roggendorf calculated that the efficacy of planimetric Z-plasty, measured as the fraction of skin elongation to scar elongation, exceeds that of the classic Z-plasty by 28%.28 In practice, it is challenging to predict the elongation effects due to patient and site characteristic differences. Nevertheless, it is advantageous that some parts of a scar can be excised by execution of planimetric Z-
plasty. This approach is useful in the treatment of irregular scars with mild contracture.
Another Z-plasty variant is the spider procedure design. It converts a skin defect to an equilateral triangle with closure by five flaps harvested from the neighboring skin in a double-opposing Z-plasty manner (Fig. 27-10). 29
The Z-plasty aims to improve the appearance of the scar, relieve tension during wound closure, and correct scar contractures (Figs. 27-11 to 27-13). In the treatment of scars and contractures, the most appropriate design must be selected from the many options available to the dermatologic surgeon. It has been suggested that the greatest advantage of the Z-plasty is replacement of an existing unattractive scar opposing RSTLs with a new scar which conforms to these lines,30 though not all evidence
supports this notion.15
The evaluation and planning of the Z-plasty procedure is influenced by more than simple geometry.17 Outcome predictions are a combination of formulaic skin biomechanics and intuition. Though the principles of flap dynamics are a function of skin mobility and deformability under tension, differing skin extensibility, or laxity, impacts the end result. Clinical studies by Gibson and Kenedi showed lengthening ranged from one-third less to two-thirds more than expected from their geometric calculations.31 This large degree of variability points to the fact that geometry alone is not a predictive measure of outcomes. Other studies have demonstrated similar findings.32–34
Complications
Though Z-plasty is a useful tool, complications do occur. The manipulated skin can be vulnerable to flap necrosis and hematoma formation, the former of which is common in Z-plasty with angles less than 30 degrees and with flap tips which necessitate frequent handling.17,35 Therefore, it is best to avoid the use of Z-plasty with such acute angles and minimize direct manipulation of triangular flap tips when possible.
CONCLUSIONS
Familiarity with the Z-plasty approach provides the surgeon with a useful tool to release contracted scars and reorient scars that are not located within RSTLs. Though breaking up a long scar into smaller, less noticeable segments has been espoused as a benefit of the Z-plasty, evidence that it accomplishes this purpose is anecdotal. The Zplasty is an essential tool for the dermatologic surgeon when considering web and freemargin correction.
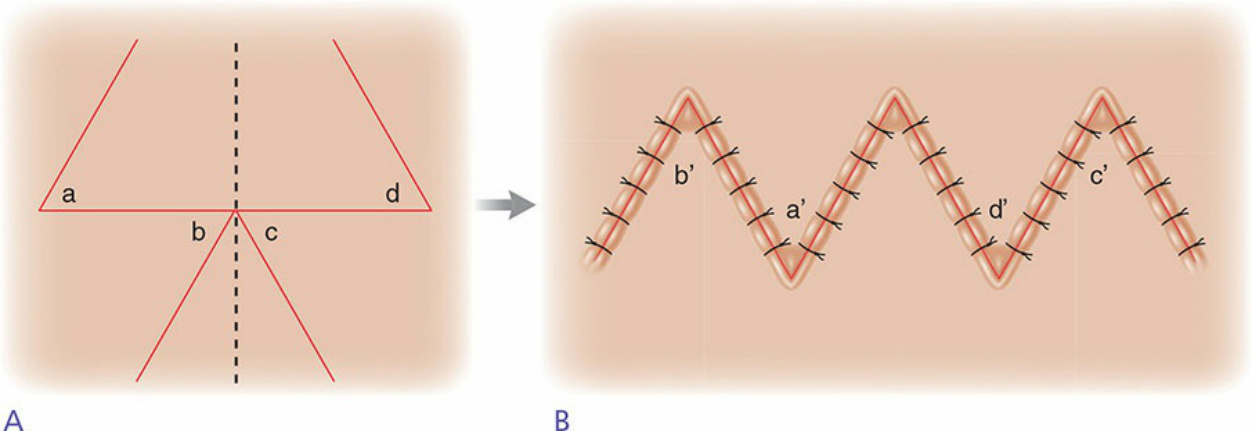
Figure 27-3. Double-opposing Z-plasty. (A) This modification consists of two mirror image Z-plasties placed immediately adjacent to one another. The dotted line represents the axis of reflection. Flap a and flap b swap positions and flaps c and d engage in a similar exchange. (B) The final result of the transposition. Since this application is primarily utilized in areas of limited skin availability, laxity, or vascularity, it is most useful in the treatment of scar contractures, webs, or burns.
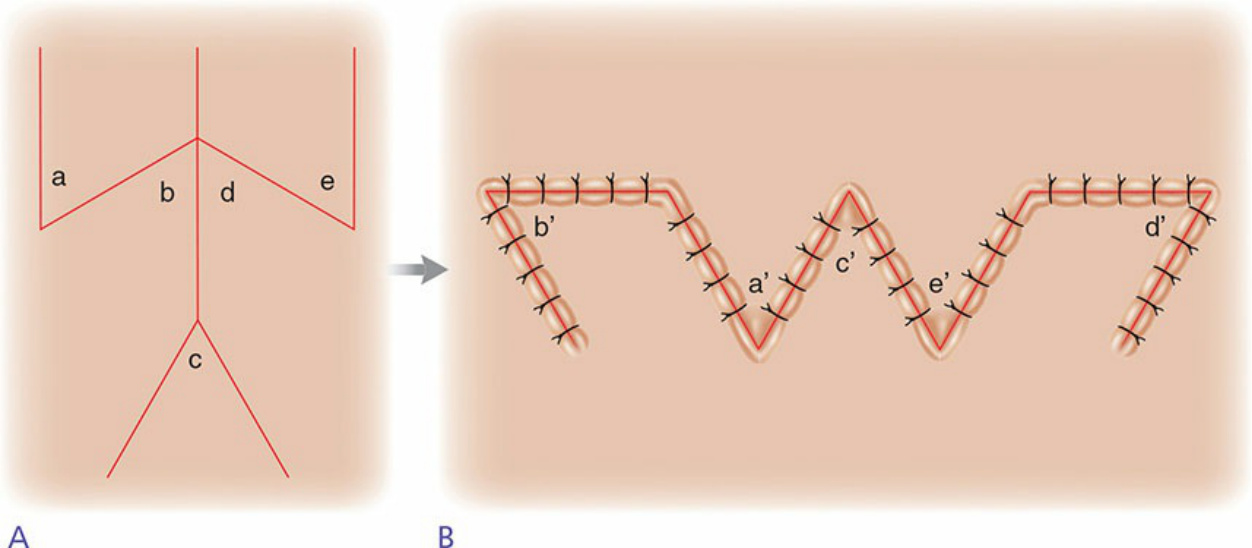
Figure 27-4. The dancing man. Mustarde’s design shares components of the double-opposing Z-plasty. Note that the Z-plasties share a common limb.
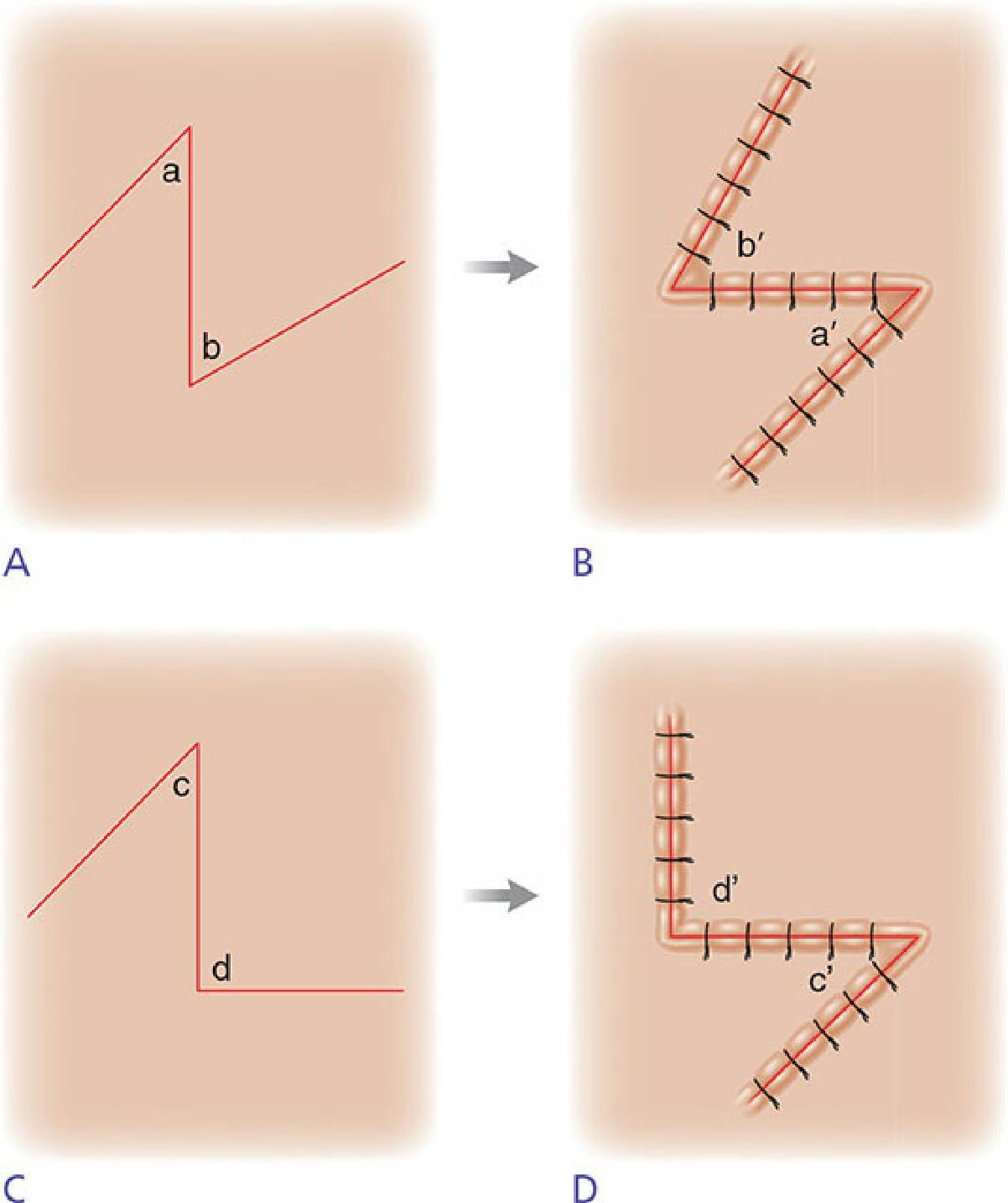
Figure 27-5. The unequal triangle Z-plasty. (A) Flaps are often designed to suit the area of reconstruction. Here, the flap angles vary. (B) The flaps swap positions, and the final placement is illustrated. (C) The half-Z-plasty is a modification of the unequal triangle Z-plasty whereby one of the two flaps is 90 degrees. (D) The flaps of the half-Zplasty undergo transposition. Note that the unequal triangle Z-plasty is useful in areas where small amounts of tissue need to be moved with as little distortion as possible such as near the eyes or lips. This Z-plasty technique is particularly useful in areas where normal skin elasticity varies such as the eyebrows.
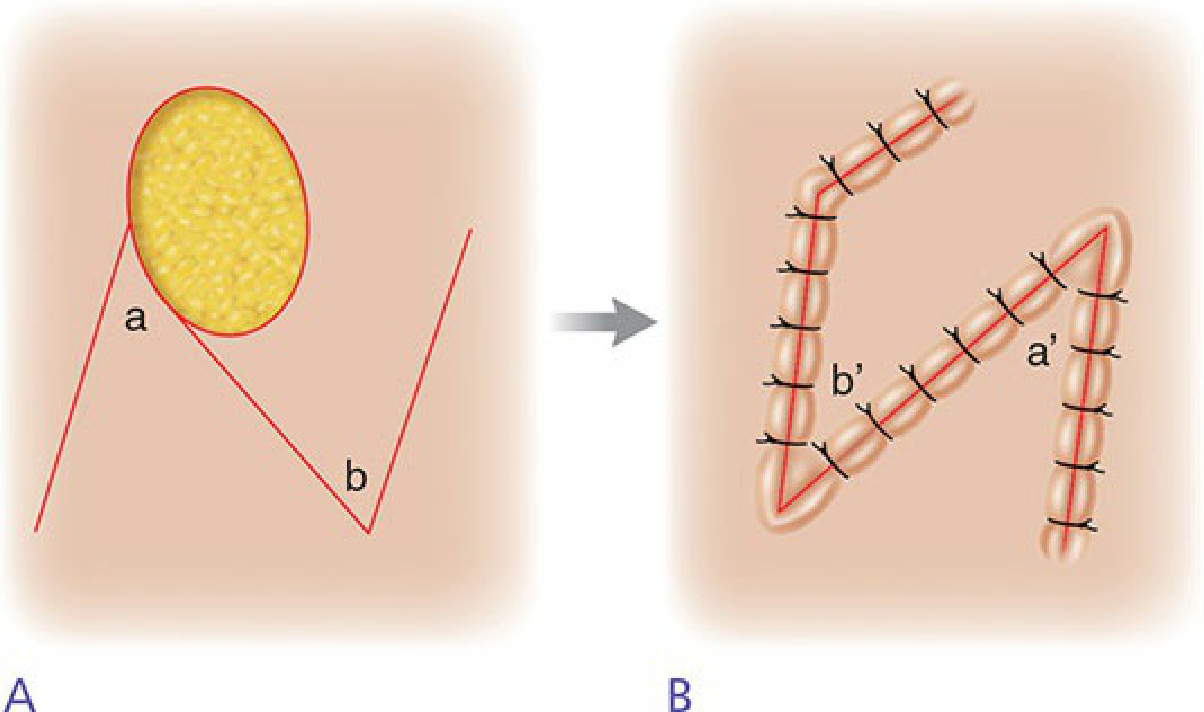
Figure 27-6. The reading man. (A) A modification of the unequal Z-plasty utilizes flap transposition to repair circular defects. (B) The outcome of the triangular flap exchange. The reading man has been utilized in the repair of large circular defects (1.5–14 cm in diameter) on the face and trunk.
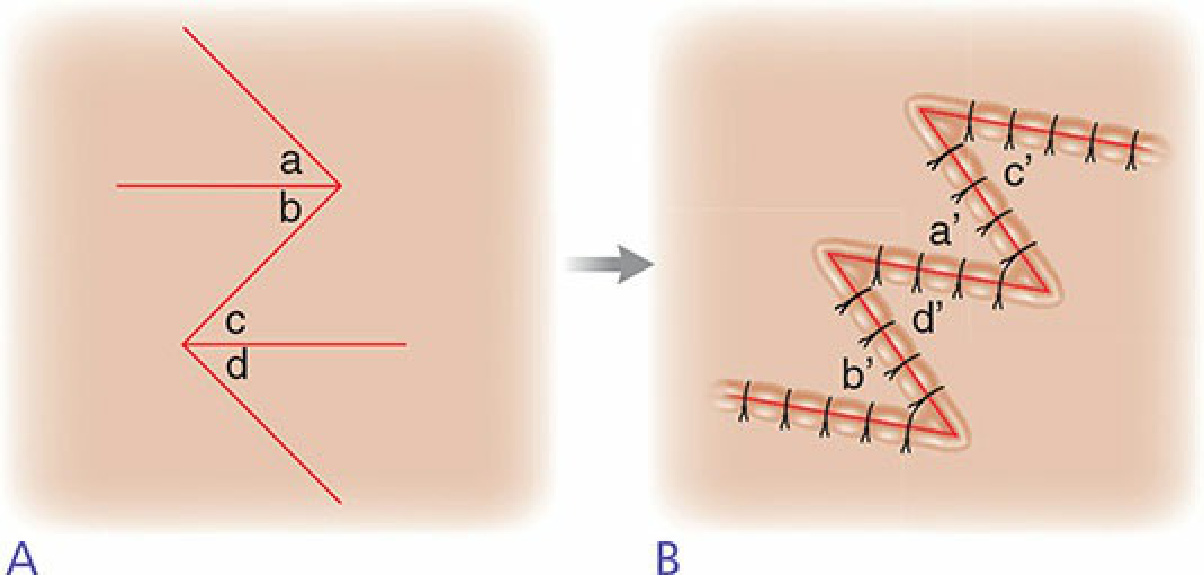
Figure 27-7. Four-flap Z-plasty. (A) An illustration of the four-flap Z-plasty shows 90-degree angles bisected into 45 degrees. (B) After flap transposition, each flap interdigitates with one another. The four-flap Z-plasty is commonly utilized in the release of web-space contractures.
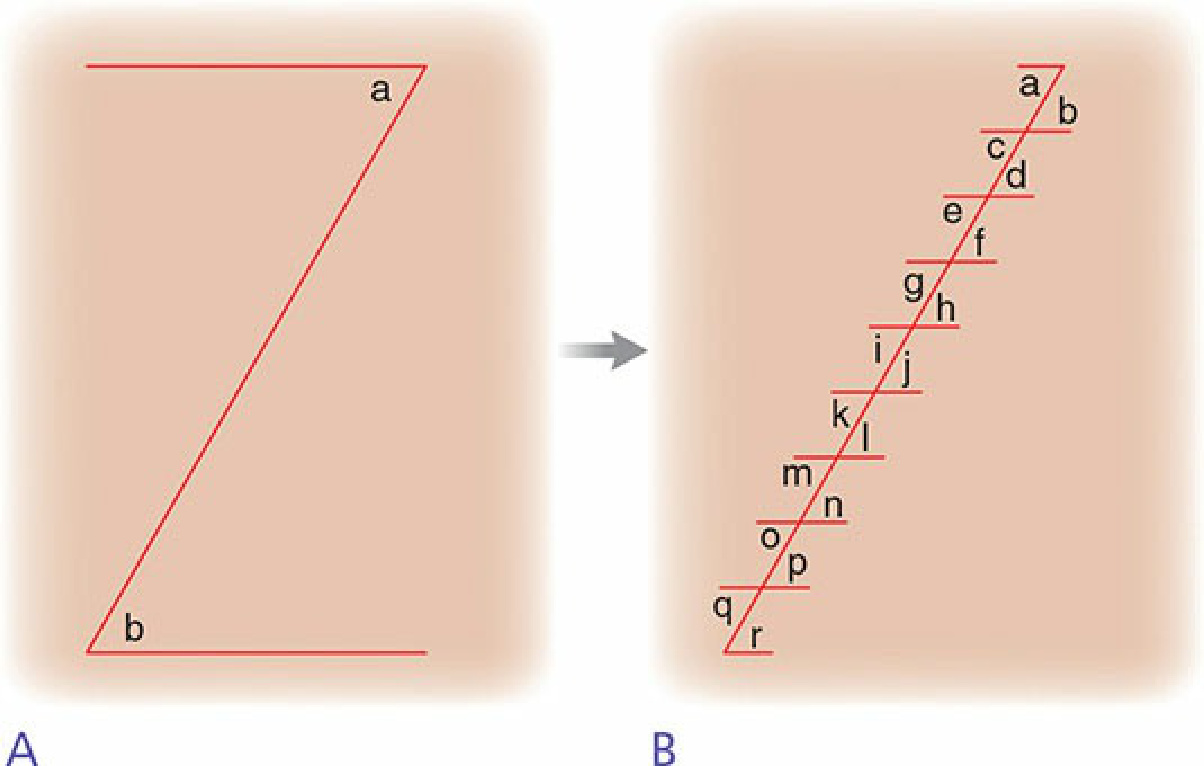
Figure 27-8. Multiple Z-plasty. (A) With longer linear scars, significant tension is substantial at the diagonal and arms of the Z, oftentimes decreasing the value of the single Z-plasty. (B) In the multiple Z-plasty, a long linear scar is divided into smaller segments each of which undergo separate Z-plasty, distributing the tension across many smaller transverse diagonals.
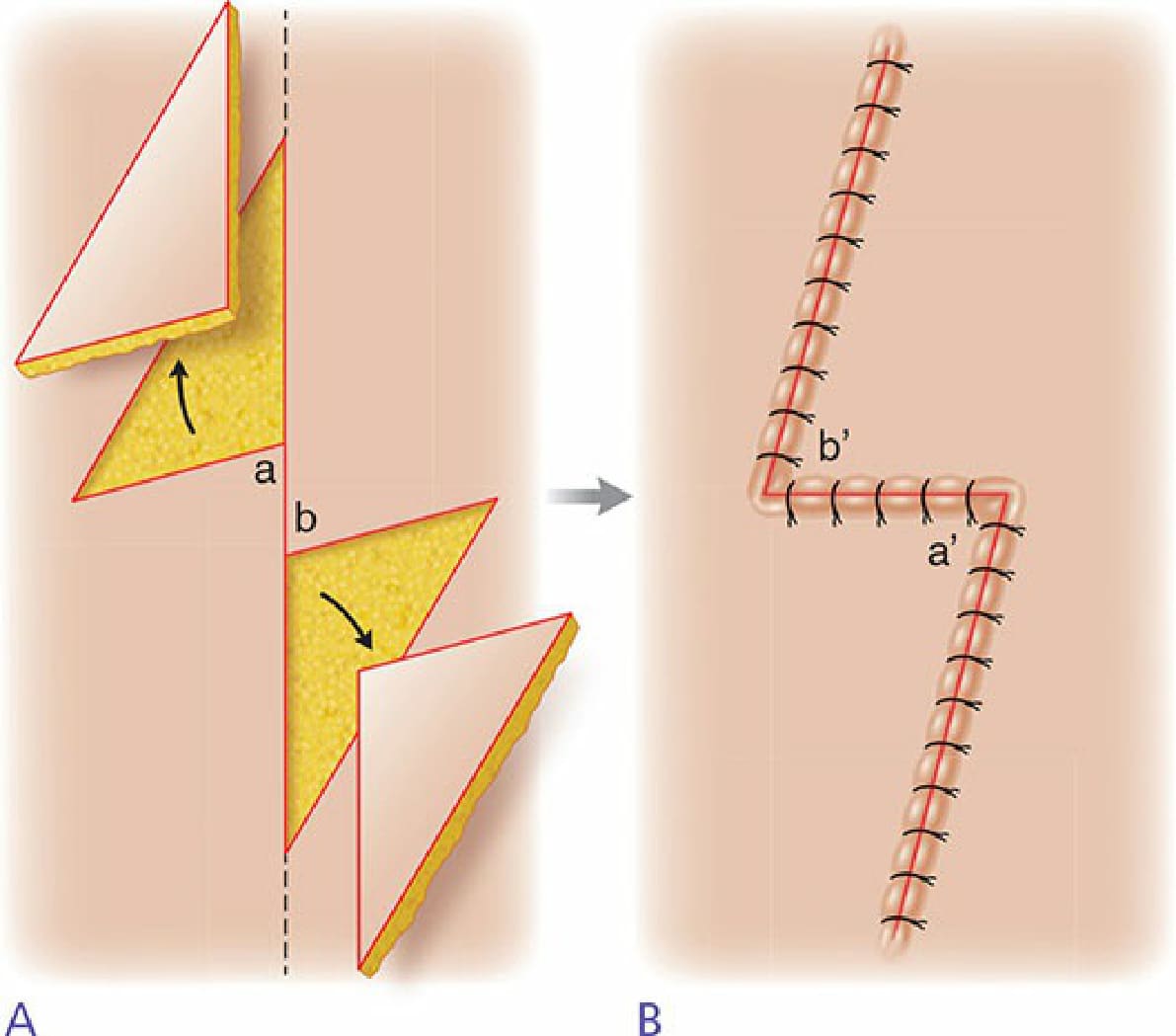
Figure 27-9. Planimetric Z-plasty. (A) 75-degree angles are utilized in this version of the Z-plasty. Limb incisions are twice the length of the central incision. Once the central incision is extended in both directions, two triangular areas are excised. (B) The effect of flap transposition. This technique is useful for correcting scars on flat surfaces and helps to avoid the elevations and depressions that can form with other types of Z-plasty, thereby creating smooth elongation of the skin along the scar axis.
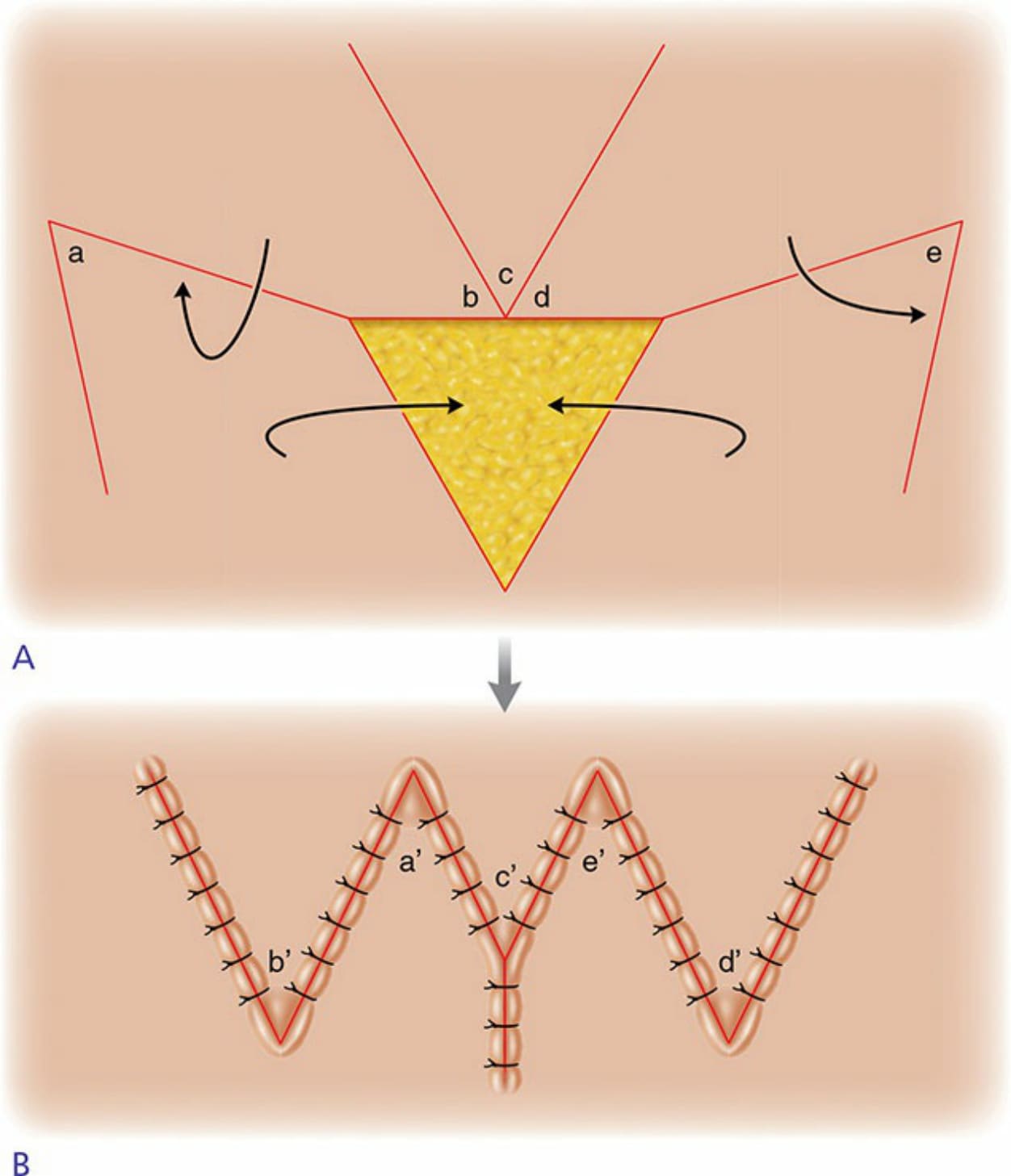
Figure 27-10. The spider procedure. (A) The illustration presents a triangular defect and incisions, which result in the formation of five flaps. Arrows signify the directions of the planned transpositions to repair the triangular defect. (B) The diagram is a representation of the final result of the spider procedure, after all flap transpositions take place. After converting skin defects to equilateral triangles, this technique can be utilized in the closure of defects in high-tension locations.

Figure 27-11. Z-plasty utilization in web correction. (A) Postprocedure photo of a primary defect near the medial canthus. (B) The photo illustrates the late sequelae of scarring near canthal folds. Oftentimes, treated lesions near the medial canthi predispose to surgical webs. (C) Medial and lateral canthal webs can be corrected with Z-plasty. Superimposed “Z” represents the required incisions for surgical correction. Note that the central limb of the Z overlies the primary problematic tension band. (D) After the flaps undergo transposition, tension is relieved. (E) A photo of the web repair with Z-plasty as noted during his follow-up appointment.

Figure 27-12. Z-plasty utilization in medial ectropion repair. (A) Photographic illustration of a left medial ectropion. (B) Mapping of vectors for Z-plasty with surgical marker ink. (C) After the incisions are performed, triangular flap transposition occurs for proper execution of the Z-plasty technique. (D) Postprocedure photo representing the final result of the Z-plasty technique in the repair of a medial ectropion. Note the presence of a Frost suture for stabilization. (E) Photo of ectropion repair with Z-plasty as documented during patient’s follow-up appointment.

Figure 27-13. Scar contracture repair and eyebrow asymmetry treated with Z-plasty. (A) Photograph of left malar eminence scar contracture in female patient. Also note patient’s eyebrow asymmetry. (B) Mapping of a multiple Zplasty across the right lateral forehead to correct brow asymmetry. (C) Immediate postoperative appearance. (D) The patient at a follow-up appointment. Note the absence of scar contractures at the operative site of the Z-plasty and correction of the brow asymmetry.