The Z-plasty technique
The Z-plasty technique
The classic Z-plasty is a surgical method of scar repair which is defined by a Z-shaped incision. The method relies on the transposition of the two triangles created by the angles of the arms of the Z-incision. In other words, two equivalent triangular flaps synchronously interchange into the space previously occupied by the other (Fig. 27-1). The result of the position swap is a 90-degree reorientation of the common arm of the Z. Fundamental goals of the Z-plasty procedure include the realignment of a scar within RSTLs, or parallel to them; the lengthening of a scar; the release of a contracture by scar lengthening; and the dispersal of a scar for better camouflage.16
In its purest form, three incisions of equal length creating a Z, or its mirror image, are the integral steps in the execution of the technique. A central incision is made (in scar revision, this common limb overlies the original scar), and two adjoining limb incisions flank the central limb. It is important to note that although the surgeon has two choices for the placement of these lateral limbs, only one combination will allow for optimal cosmesis or reorientation of lines in the direction of, or parallel to, the RSTL (Fig. 27- 2).17 Therefore, each incision’s relationship to the RSTL is critical when planning Zplasty to address scar orientation.
Another important factor in successful implementation of the Z-plasty is the angle created by the central and lateral limbs. Although angles from 30 to 90 degrees are possible, the 60-degree Z-plasty is the most common. As a general rule, the 60-degree Z-plasty should reorient the central scar by 90 degrees and yield a 75% increase in the length.
Classically, the Z-plasty consists of three equivalent incisions at 60-degree angles (Fig. 27-1). The central incision often overlaps the long axis of the scar, or alternatively the site of the defect if the scar is excised. After undermining the surrounding skin, the resultant triangular skin flaps are freed from the subcutaneous plane which lies below. The triangular flaps are then exchanged so that the shared side of the triangles now lies against the skin of the lateral limb incisions and the resultant central limb is reoriented in a perpendicular fashion, ideally now parallel to RSTLs.
The Z-plasty procedure should not be used for every scar revision. If a scar already lies along RSTL, a Z-plasty may result in reorientation of the central incision perpendicular to the RSTL, typically a less desirable outcome. Similarly, scars within 40 degrees of RSTLs might be better managed with simple excision than with Zplasty.18 Large Z-plasty approaches should generally be avoided given the substantial tension vectors that may exist across their common limbs; in such cases, multiple Zplasty, as detailed below, would be preferable.
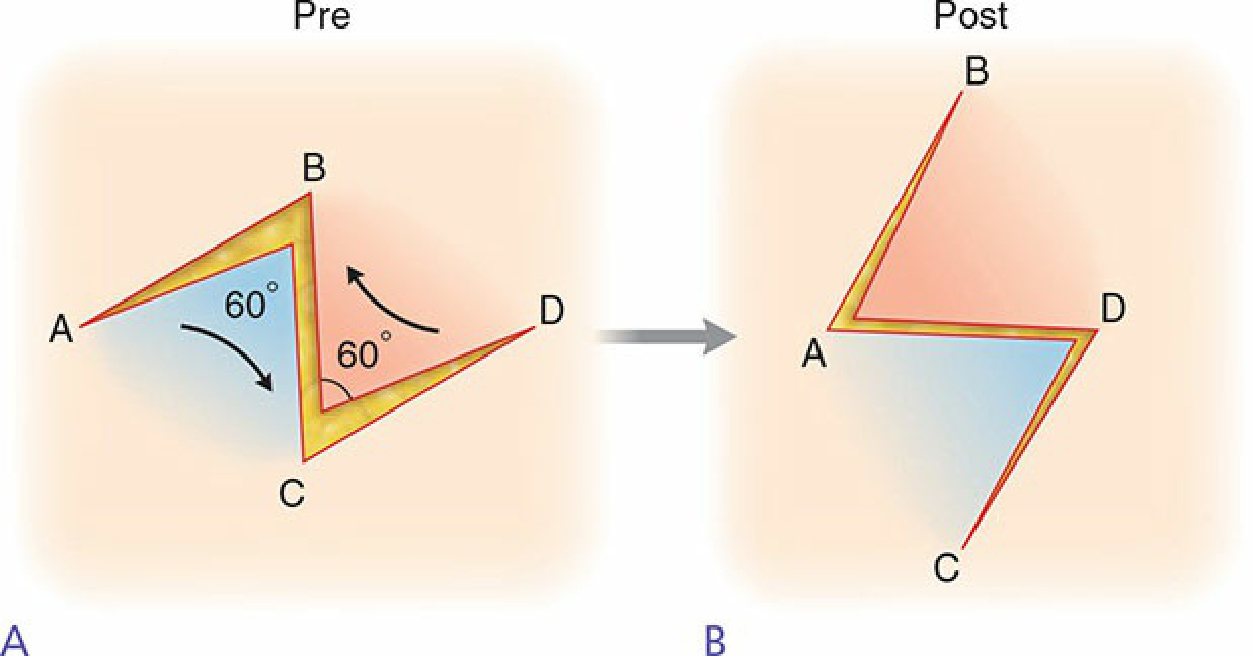
Figure 27-1. The classic Z-plasty. (A) The central limb of the original Z-plasty overlies the original scar. (B) After transposition of the triangular flaps created by the Z-plasty, the central limb is reoriented perpendicular to the original scar and parallel to the relaxed skin tension lines.
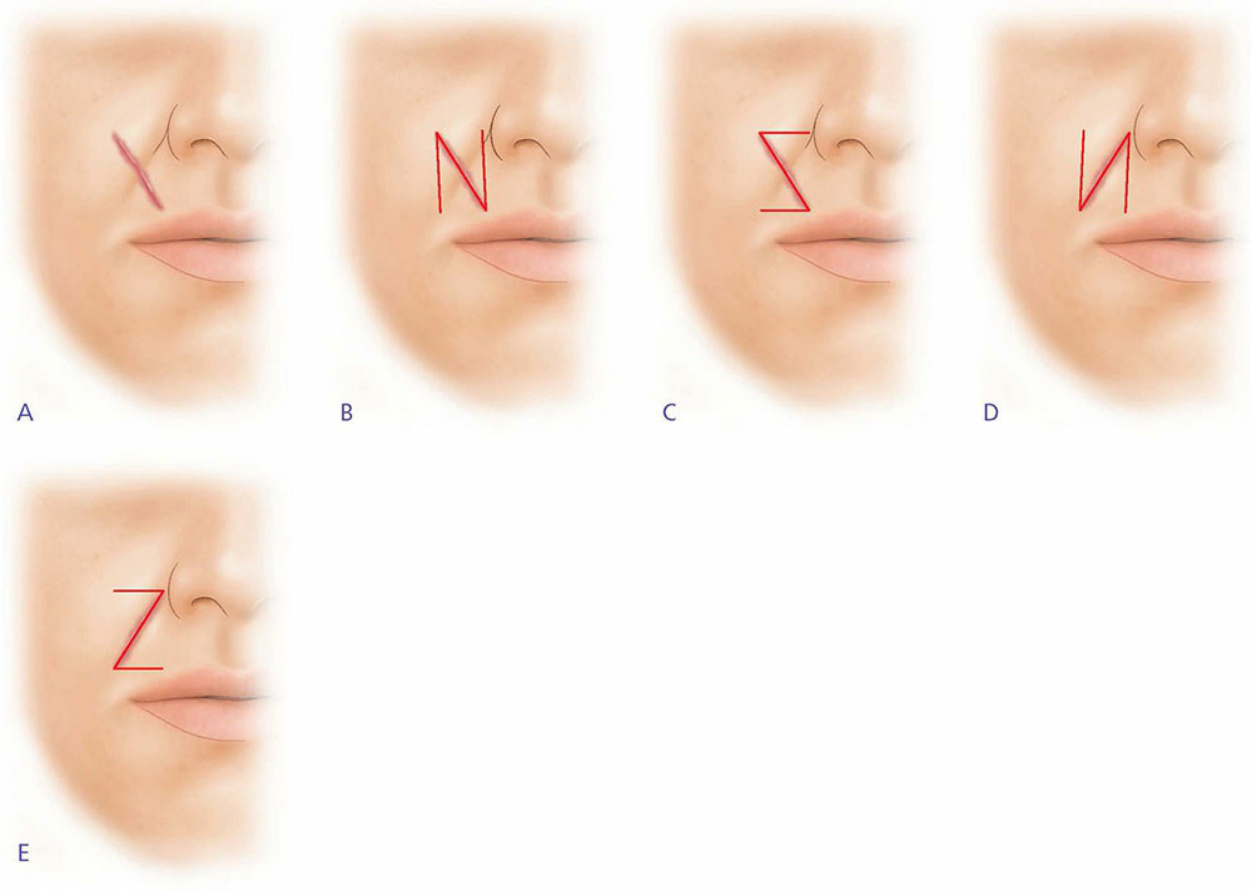
Figure 27-2. Z-plasty can reorient a scar 90 degrees. (A) A scar is oriented perpendicular to the right melolabial fold. (B) One choice for the Z-plasty is an incision line that lies over the original scar line and two adjacent vertical lines that serve as the limbs of the complete Z-plasty. (C) The other option for the Z-plasty is an incision line that overlaps the original scar and two horizontally placed incisions. (D) This figure represents the outcome of the transposition which takes place after the two triangular flaps in figure B exchange positions. The central limb now lies within the melolabial fold, now 90 degrees to its original position. Moreover, the two vertical incision lines fall within relaxed skin tension lines. This choice is favorable. (E) This figure represents the outcome of the transposition which takes place after the two triangular flaps in figure C exchange positions. Here, the horizontal incisions will not fall within the relaxed skin tension lines, essentially creating scars which will not hide within the natural contours of the facial lines. Note that both designs will reorient the original scar 90 degrees, to a position within the melolabial fold. However, one choice is clearly better than the other.