Therapeutic pearls
Therapeutic pearls
Lymphedema is a common problem in this area, and persists for many months. Ectropion can result from lower eyelid laxity, and a lid-tightening procedure may be warranted. Entropion of the upper eyelid can occur, allowing hair and skin to touch and irritate the cornea. Ensuring the new anterior lamella is firmly attached to the cartilage or free tarsal graft can help prevent this. Given the morbidity and potential complications of this repair, it should be reserved for large defects when other reconstructive options have been deemed unsuitable. A modified Cutler–Beard flap with earlier pedicle division has been described.24 In this procedure, a free tarsal graft is harvested from the contralateral upper eyelid and sutured to the posterior lamella and levator aponeurosis. A skin-only flap is created on the lower lid, and is elevated and sutured in a manner similar to the traditional Cutler–Beard flap. The pedicle is divided at 2 weeks and returned to the lower eyelid. The authors describing this technique found no cases of necrosis or entropion, though one patient had ectropion (Fig. 14A–J).24
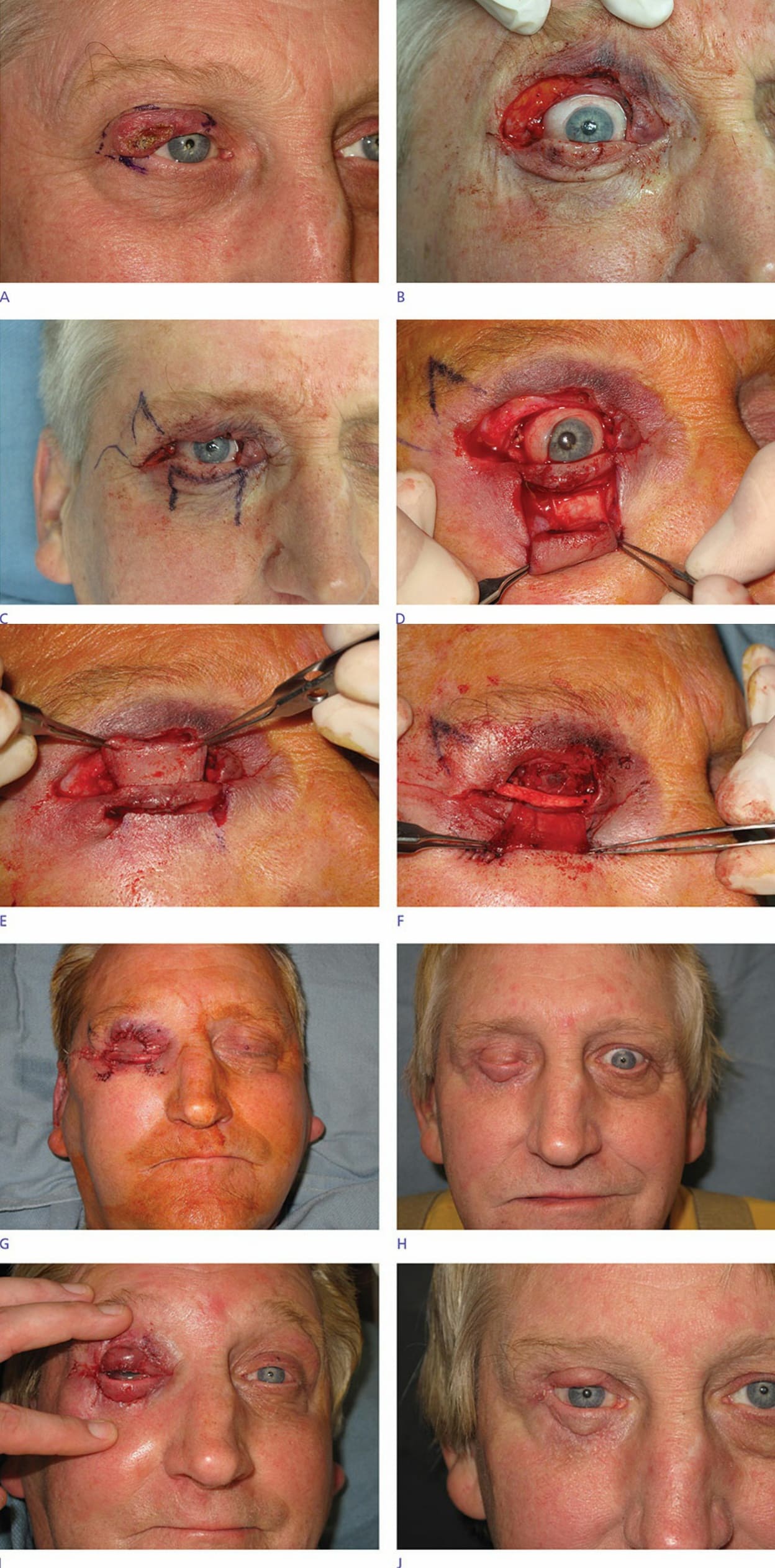
Figure 26-14. (A) Tumor on right upper eyelid. (B) Full-thickness upper eyelid defect following Mohs micrographic surgery. (C) Template drawn on lower eyelid. (D) Flap incised and elevated. (E) Flap passed under the tarsal plate. (F) Cartilage graft placed for structural support. (G) Flap sewn in place. (H) Flap survival at follow-up 10 weeks later. (I) Pedicle divided. (J) Postoperative appearance at 1 month.