Technique pearls
Technique pearls
Flattening of the melolabial fold occurs as a result of this flap, though this is usually mild and not bothersome to the patient. If needed, an elliptical excision of the contralateral melolabial fold can recreate symmetry.
Necrosis may be seen more often with the CIF compared to other interpolation flaps due to its less robust blood supply. When this occurs, it most often involves the distal edge of the flap which can be left to heal by secondary intention. These flaps also have a tendency to pincushion, which may be of benefit to restore the convexity of the ala. If it is problematic, intralesional triamcinolone can be used starting approximately 1 month after takedown. All patients should be counseled that additional revisions such as dermabrasion or contouring may be required at a later date (Fig. 11A–G).
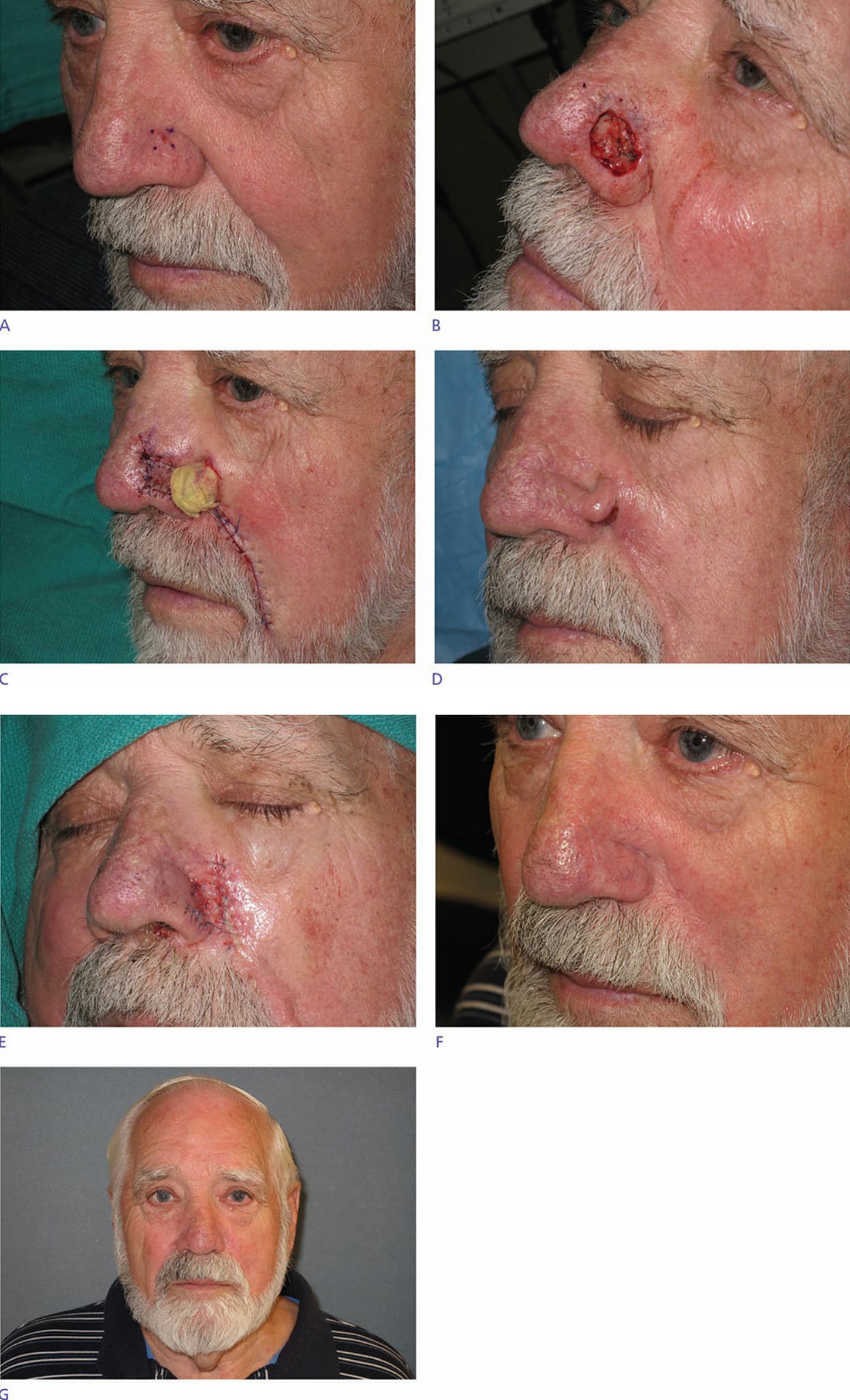
Figure 26-11. (A) Basal cell carcinoma on the left nasal ala. (B) Defect following Mohs micrographic surgery. (C) Flap sewn into place and pedicle wrapped with Surgicel and Xeroform gauze. (D) Flap survival at 3 weeks. (E) Pedicle division and inset. (F) Postoperative appearance at 6 months (oblique view). (G) Postoperative appearance at 6 months (frontal view).