Technique pearls
Technique pearls
The surgeon should precisely design a template that accounts for the three-dimensional shape and contour of the nose (Fig. 9A,B). It is best to match the thickness and contour as much as possible during the initial inset, though a delicate balance must be maintained as aggressive thinning in the first stage may increase the risk of ischemia. An oversized flap, or a flap that has not been appropriately thinned, may require a revision with another surgery, intralesional steroids, dermabrasion, or laser. This is often addressed 4 to 6 months from flap takedown.
Surgeons should also devote time to repairing the secondary defect on the forehead to prevent a noticeable, inverted scar. If tension is too great, the area should be left to heal by secondary intention.
Paresthesias secondary to transection of the supratrochlear nerve can be permanent and patients should be counseled about this prior to surgery.
Necrosis is rare given the reliable blood supply to this flap, though it may occur in the setting of extreme tension or if the patient is a heavy smoker. Superficial slough can be removed at the time of division and left to heal by secondary intention. In the catastrophic event of complete flap failure, observation is recommended. The pedicle will autoamputate and revisions can be performed at a later date if needed. In general, this flap approach is reliable and leads to excellent aesthetic and functional outcomes (Fig. 10A–M).

Figure 26-9. (A,B) The three-dimensional template is carefully removed to keep its shape. Relaxing incisions are made to flatten the template prior to transferring onto the forehead.
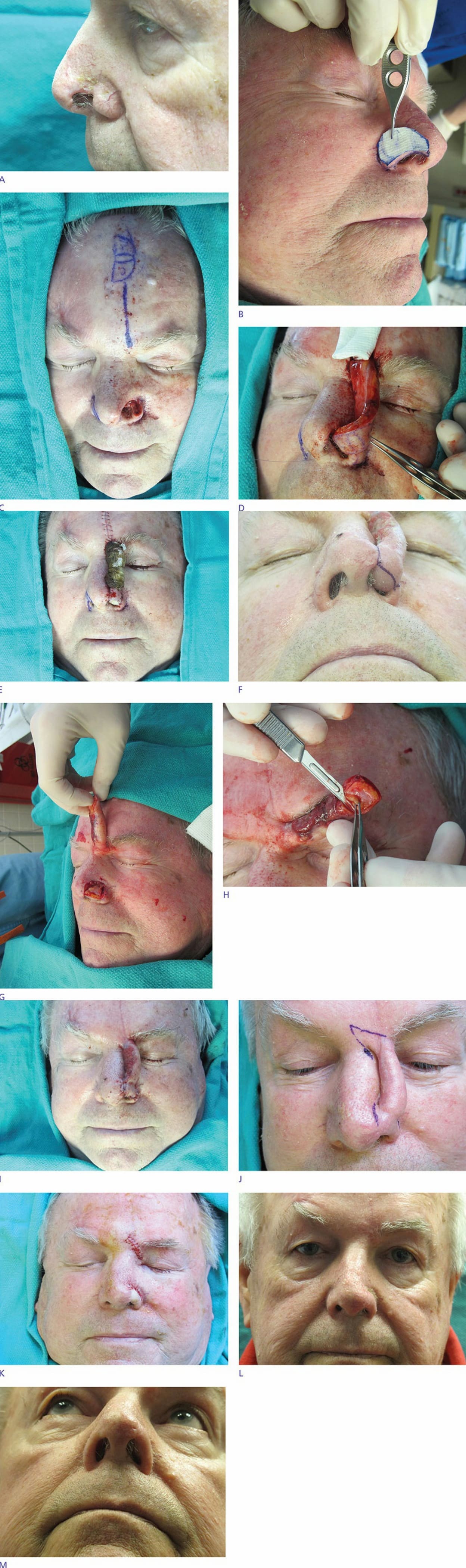
Figure 26-10. (A) Full-thickness defect on the left nasal ala following Mohs surgery. (B) Template made from contralateral ala. (C) Template inverted onto forehead. (D) Fold-over flap used to recreate nasal lining. Pedicle wrapped with Surgicel and flap sewn into place. (F) Return for the second stage 3 weeks later with planned division at the alar rim. (G) Pedicle divided at the alar rim and internal lining visible. (H) Pedicle and internal lining are thinned appropriately. (I) Pedicle is resutured. (J) Return for the final stage 3 weeks later (6 weeks from stage 1). (K) Division of pedicle performed. (L) Postoperative appearance at 1 month (frontal view). (M) Postoperative appearance at 1 month (inferior view).