Design
Design
Choosing the appropriate wound and location is the first step to success when executing this flap. It is important to assess the amount of mobility that will be produced when circumferential margins of the island are severed. Although this flap can be used for defects ≥2 cm in diameter on cosmetically sensitive areas such as the nose or upper lip, the island pedicle flap is typically suited for small- to medium-sized wounds on these areas. The nose has stiff skin and typically lacks the compliance and pliability of other areas such as the cheek. Moreover, due to the curvature of the numerous nasal cosmetic subunits, secondary motion may lead to cosmetically undesirable nasal asymmetry.
Proper design is crucial to the execution and outcome of the island pedicle flap, and
allows the surgeon to achieve optimal and reproducible aesthetic results with minimal risk. In general, the flap is designed as an isosceles triangle with two longer edges (the sides) and one shorter edge (the base). The long axis of the flap is ideally placed in relaxed skin tension lines and may be curvilinear to match areas such as the melolabial fold or the vermillion border. This allows the healed incision scars to hide within natural skin folds, making them less cosmetically distressing.
In its classic design, the flap is incised adjacent to the defect and within the same cosmetic subunit (Figs. 25-3 and 25-4). The flap is oriented tangentially away from the defect. The length of the triangular pedicle is usually three to four times the width of the defect, with the apex of the isosceles triangle is angled at roughly 30 degrees. Incisions around the triangular island are made to the level of the subcutaneous fat. The pedicle is also incised with vertical incisions deep to the subcutaneous tissue and may contain muscle or superficial musculoaponeurotic system (SMAS) elements. The surgeon should be comfortable with anatomical variations of structures, and particularly vessels in all layers of the subcutaneous tissue. Even if the flap is overlying a named vessel, this vessel is not dissected with the flap, as the pedicle provides a rich enough vascular subcutaneous plexus to maximize chances of flap survival.
Critically, the flap should be slightly undersized for the defect.15 Thus, the width of the flap is ideally slightly smaller than the width of the defect. This requires secondary movement of tissue around the defect, but reduces the risk of flap protuberance after it has healed. Basting sutures may also be used to mitigate the risk of trapdoor formation.
The flap is next undermined along the edges, but not at the base of the pedicle. The surrounding skin of the primary surgical defect is also undermined at the same level. The tissue of the pedicle is left intact without excessive undermining to allow for adequate, random pattern perfusion from the subcutaneous plexus. If inappropriately undermined, the flap is at risk of failing due to a compromised vascular supply needed to nourish the tissue. The pedicle itself can contain epidermis, dermis, subcutaneous tissue, fat, muscle, and parts of the SMAS. Undermining of the surrounding edges is performed above the superficial fascia, allowing for adequate movement. This minimizes tension with wound closure and helps to prevent inversion caused by pull at the leading edge. In some areas, such as along the eyelid margin, the secondary motion created by the flap can cause undesirable functional or cosmetic results, such as ectropion.
After freeing the island, the flap should be advanced forward into the primary defect
in a V-Y manner. While advancing the flap, secondary tissue movement will be necessary, especially given the bulky nature of the pedicle. This motion of pulling the flap forward also allows the surgeon to visually determine which aspect of the flap requires more mobility. If the surgeon places a finger on the pedicle during movement, the remaining vectors of resistance may be determined and additional undermining may be performed to free up movement in this vector. The narrow tail of the flap is often an area that requires additional undermining to lessen restriction on the advancement of the pedicle. Aggressive undermining of the apex, or the tail, can significantly improve the mobility of the flap.
If the pedicle itself requires undermining, this is done with extreme care. The surgeon should test flap mobility after each step of undermining to minimize overundermining the pedicle and compromising its vascular supply. Usually, the leading edge of the flap is also undermined, but to a lesser degree than the tail.
The key suture of this flap is placed in the deep dermis at the midpoint of the leading edge and the corresponding point of the defect. Buried vertical mattress or set-back sutures are ideally used.15 Tip stitches for the apex of the flap are generally not necessary. Basting or quilting sutures may be used to tack down the body of the flap, though care should be taken to avoid ligating the flap’s vascular supply. After all dermal sutures are placed, the elevation of the pedicle should be lower than that of the surrounding skin, perhaps by as much as 2 to 3 mm. With wound contraction and healing, the pedicle will elevate relative to the position of the surrounding skin.
Due to the nature of the design with free margins on all sides of the pedicle, this flap is particularly susceptible to the trapdoor phenomenon, producing a protuberant aesthetic appearance (Fig. 25-5). This complication commonly develops early during the postoperative period, and occurs more often on the medial cheek or lip. Undersizing the flap will help to minimize the trapdoor deformity, although this requires secondary motion of the edges surrounding the defect. The surgeon must account for and predict this secondary motion in order to properly execute the flap.
The classic locations chosen for repair using the island pedicle flap include the upper lip. Other areas for which this flap can be used include the upper brow/temple, lateral upper lip, medial cheek (Fig. 25-6), upper nasal dorsum, and alar groove. Some of these locations may require the use of a modified flap design.

Figure 25-3. Classically, the flap is designed to stay within the same cosmetic subunit.

Figure 25-4. The tail of the flap may ideally be hidden along cosmetic subunit boundaries.

Figure 25-5. Pincushioning, or the trapdoor phenomenon, is classically see with this design.
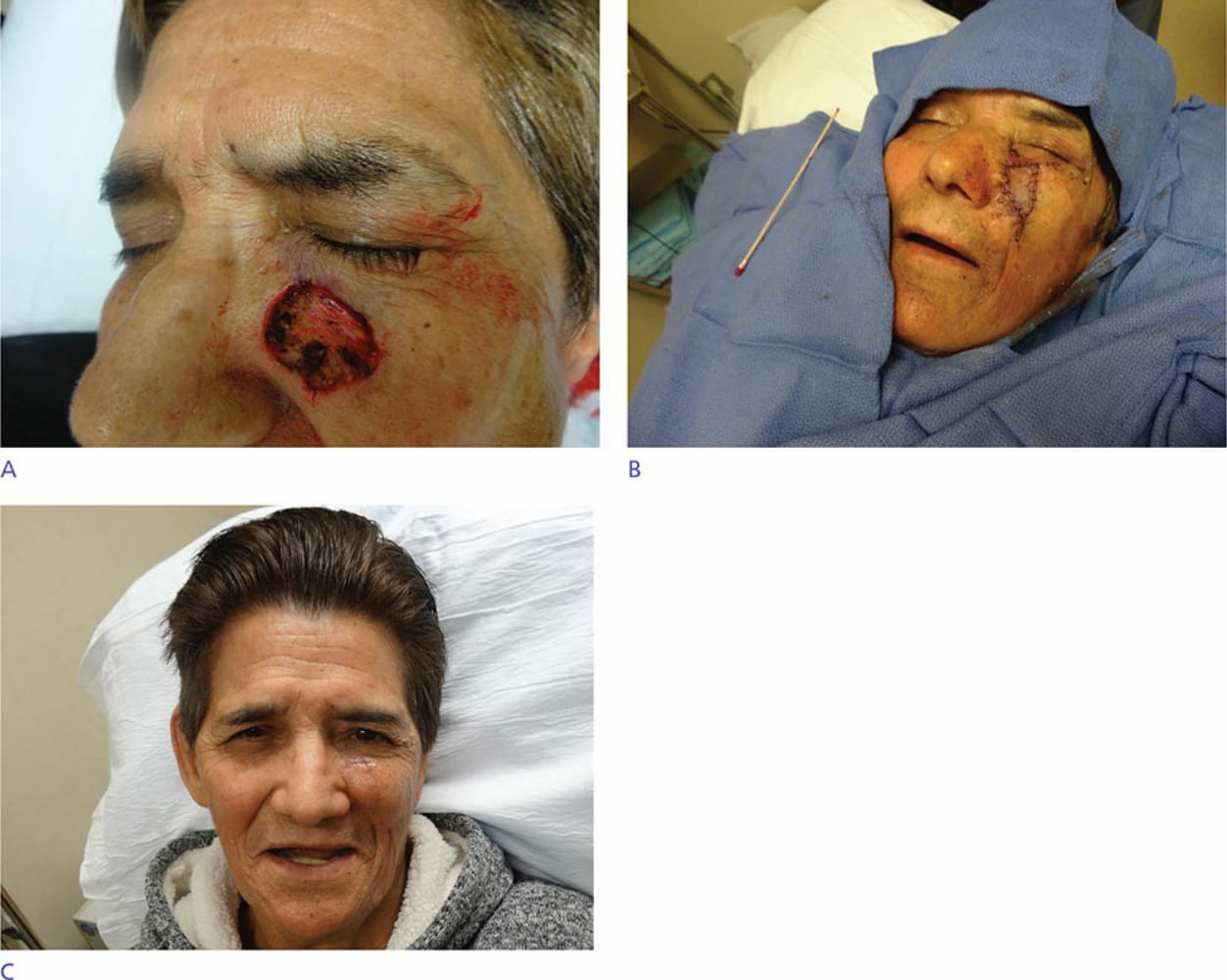
Figure 25-6. This flap may be used beyond the lip and nose, and cheek defects can be reliably reconstructed as well.