Trilobed flap
Trilobed flap
The most common variation on the bilobed flap is the trilobed flap. When faced with a defect where there is little tolerance for tension on the surrounding skin, a bilobed should be considered; when a bilobed design presents challenges, consider the trilobed flap (Fig. 24-4).15
A trilobed flap may be a viable option for distal nasal defects, such as those on the infratip. Beginning at the defect, draw similarly sized lobes until the final lobe is pointing exactly vertically. Though the additional lobe will cause the total angle of flap transfer to increase, each lobe is only rotating 45 degrees or less. Therefore, a trilobed flap does not cause any additional standing cone deformity around the pivot point.
A trilobed flap with a diminutive vertical Burow’s triangle has been reported for defects on the medial ala; however, a very short Burow’s triangle with its apex in the alar crease could theoretically lead to nasal valve constriction.16 A quadrilobed flap has also been described, again for distal tip defects.17 In these cases, however, a medially based bilobed flap (as discussed below) may be a more straightforward option.
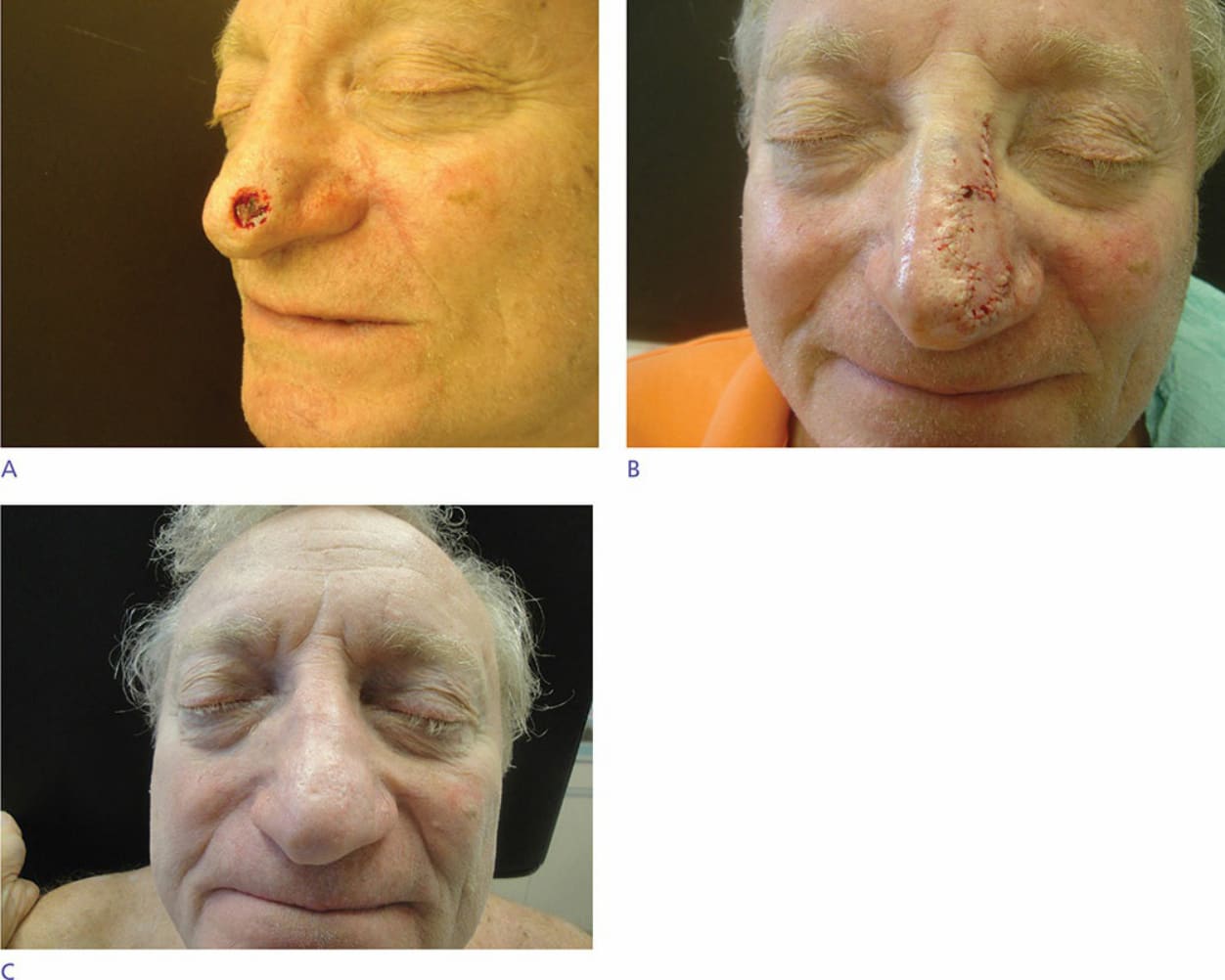
Figure 24-4. Series of photos for trilobe flap on infratip. Mohs defect (A), immediately postrepair (B), and 3 months postoperative (C).