Design principles
Design principles
To minimize the risk of distortion, the width of the secondary lobe, primary lobe, and primary defect are all designed to be of equal size (Fig. 24-2). To facilitate closure, the secondary lobe may be slightly narrower when it is located on relatively immobile skin adjacent to the medial canthus. Some authors have suggested adopting undersized primary and secondary lobes.8 This approach can be considered if there is considerable tissue laxity around the primary defect.
If the flap is meticulously designed so that the lobes of the flap equal the width of the defect, then virtually all of the flap’s tension is in closing the tertiary defect. This is analogous to a standard transposition flap closure, where the key suture—and attendant tension—is in closing the secondary defect. As such, the bilobed flap’s tertiary defect should be oriented vertically. Any diagonal vector to this final defect may cause
elevation of one of the alar rims.9
The ideal defect for the bilobed flap is small (less than 1.5 cm) and located on the lateral nasal tip or distal nasal sidewall. When performed in this location, the skin laxity of the medial cheek and nasofacial sulcus is recruited when closing the tertiary defect. In theory, however, defects of any size and in any nasal location may be repaired with a bilobed flap, as long as the flap can be drawn entirely on the nose with the final lobe pointing superiorly. The upper limit of a defect amenable to this procedure is contingent on the size of the patient’s nose, the location of the defect on the nose, and the elasticity of the nasal bridge skin. Limitations of the bilobed flap—or, at least, a realization that there is less room for error—become evident when defects are larger or arise within rigid sebaceous skin.10
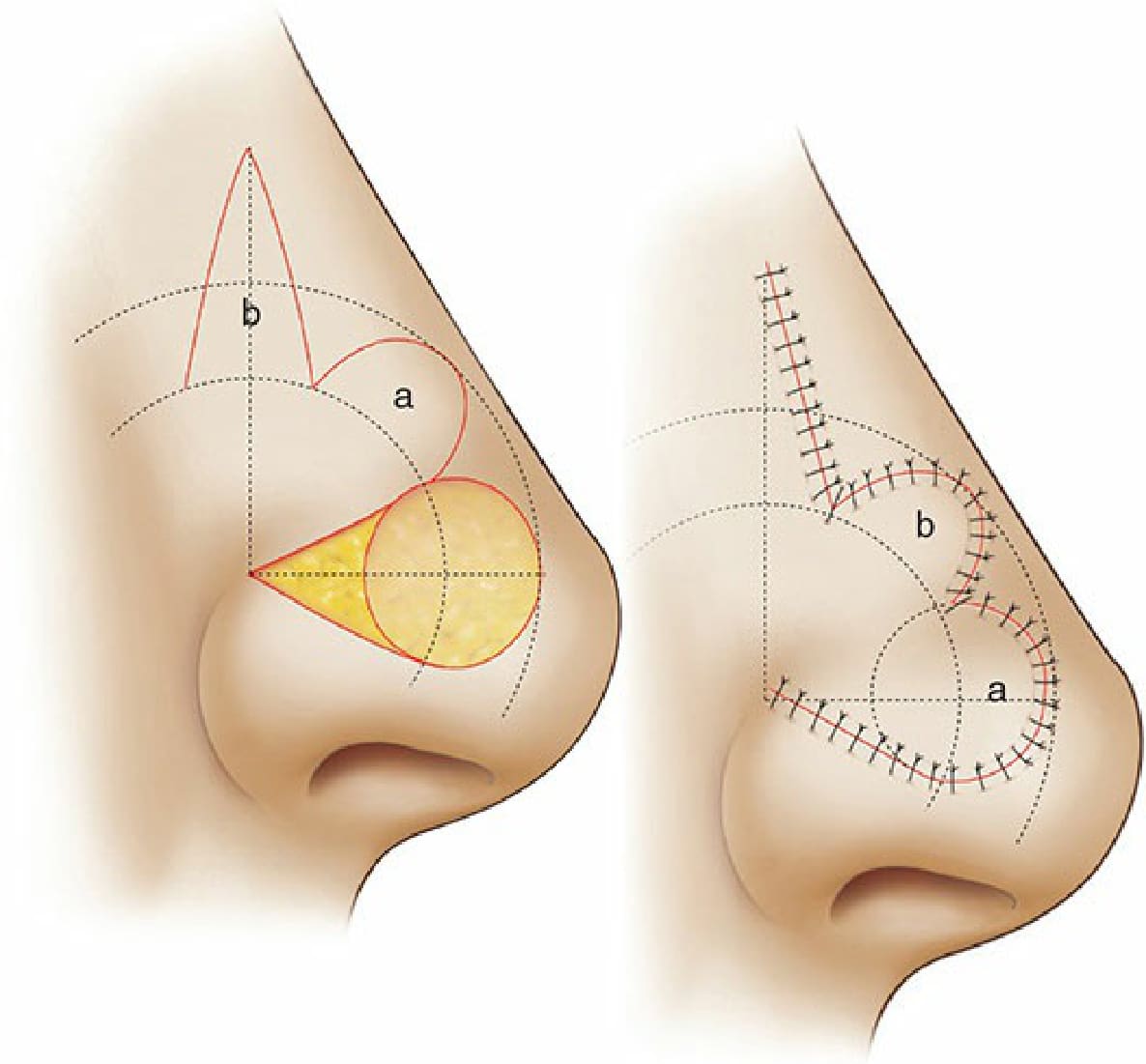
Figure 24-2. Zitelli modifications of the bilobed flap. Decreased angle of tissue transfer and incorporation of a Burow’s triangle reduces standing cone deformity. The apex serves as a focal point for the design. Each donor lobe is designed around one arc through the center of the defect, and another arc through the distal end of the defect.