Specific examples of multilobed transposition flaps
Specific examples of multilobed transposition flaps
Bilobed flap. If a rhombic flap is not possible because tension on the skin immediately adjacent to the primary defect is excessive or causes anatomic distortion, the bilobed flap can reach donor sites more remote from the defect. Compared to the rhombic flap, the geometry and execution of the bilobed flap are more complex. Excellent reviews have been written on this topic.8–11 The bilobed flap is most commonly utilized to repair wounds on the nose or near the eyelid, though it can be used in nearly any anatomic location (Figs. 23-23 and 23-24).12
Like the rhombic flap, the bilobed flap also rotates approximately 90 degrees. However, the bilobed flap distributes the rotation between the two lobes, each rotating 45 degrees. The second lobe incorporates a Z-plasty that helps to push the flap toward the primary defect (Fig. 23-25). If the primary defect is near a free margin, the tension vector to close the donor site for the secondary lobe (i.e., the tertiary defect) should generally be parallel to the free margin to preserve its position. To avoid secondary motion at a primary defect near a free margin, the primary lobe should also be sized to match the primary defect. The secondary lobe may have 85% to 90% of the surface area of the primary defect. The design details of a nasal tip defect repaired with a bilobed flap are shown in (Fig. 23-26).
The first key suture closes the tertiary defect and ideally pushes the flap toward the primary defect. The second key suture sets the primary lobe into the defect. The exact position of this suture may vary or require adjustment to create tension vectors that avoid anatomic distortion, to align the standing cone, and to adjust the sizing of the primary lobe. The secondary lobe usually has excess length and must be trimmed to match the secondary defect.
Trilobed flap. The trilobed flap has tissue mechanics similar to the bilobed flap with a few distinct advantages (Fig. 23-27). First, its third lobe allows the flap to reach tissue reservoirs increasingly remote from the primary defect, and it is particularly useful to reconstruct distal nasal defects. Second, the third lobe extends the arc of rotation to 120 to 150 degrees and may provide a more favorable tension vector to close the quaternary defect. Third, the additional lobe adds the benefit of another Zplasty, which decreases the tension to transpose the flap, an important advantage when even mild tension at the distal nose can distort the free margins. Finally, the third lobe increases the width of the flap pedicle. If the orientation of the standing cone would cut into the pedicle of a bilobed flap, the increased pedicle size of a trilobed flap can improve blood supply.13

Figure 23-23. Defect on the radial dorsal hand repaired with a bilobed flap. (A) Mohs defect. (B) Flap design. Note the more favorable location of the tertiary defect which facilitates closure. (C) Immediate postop appearance. (D) Long-term follow-up.

Figure 23-24. Defect on the right infraorbital cheek repaired with a laterally based bilobed flap. (A) Mohs defect and flap design. (B) Immediate postop appearance. (C) Long-term follow-up (14 months, treated with pulsed-dye laser).
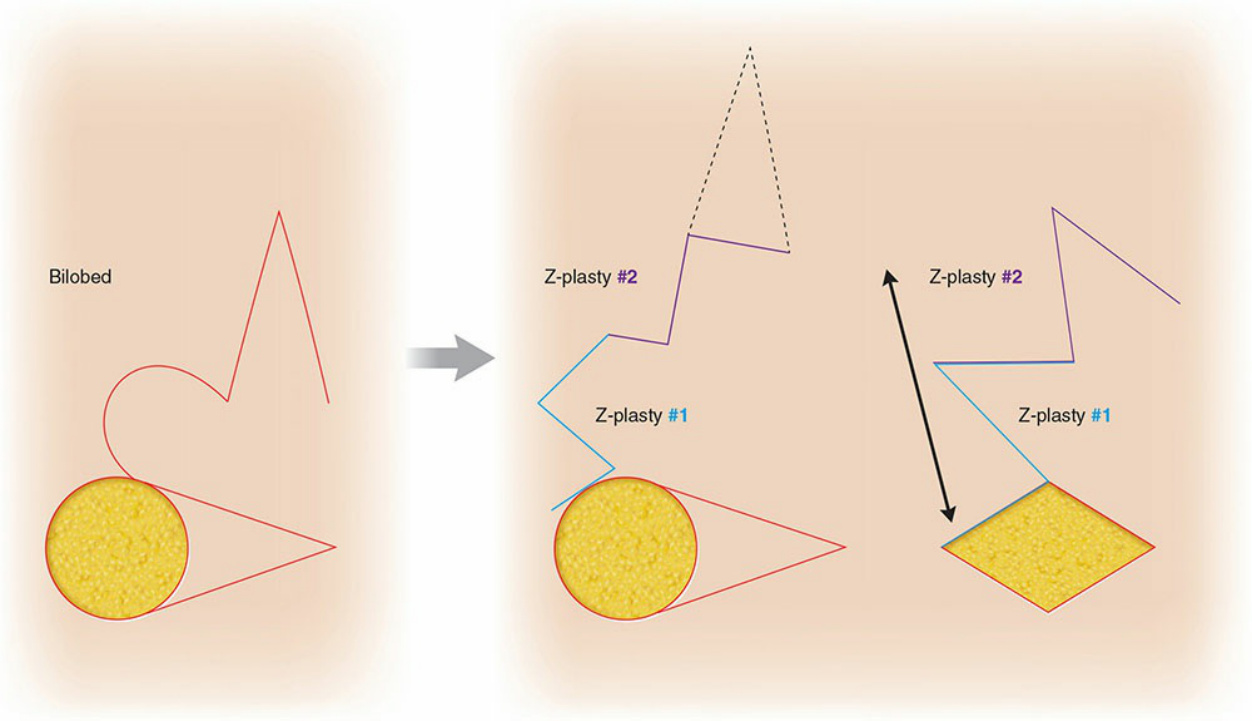
Figure 23-25. The bilobed flap represented as two consecutive Z-plasties that lengthen the flap.
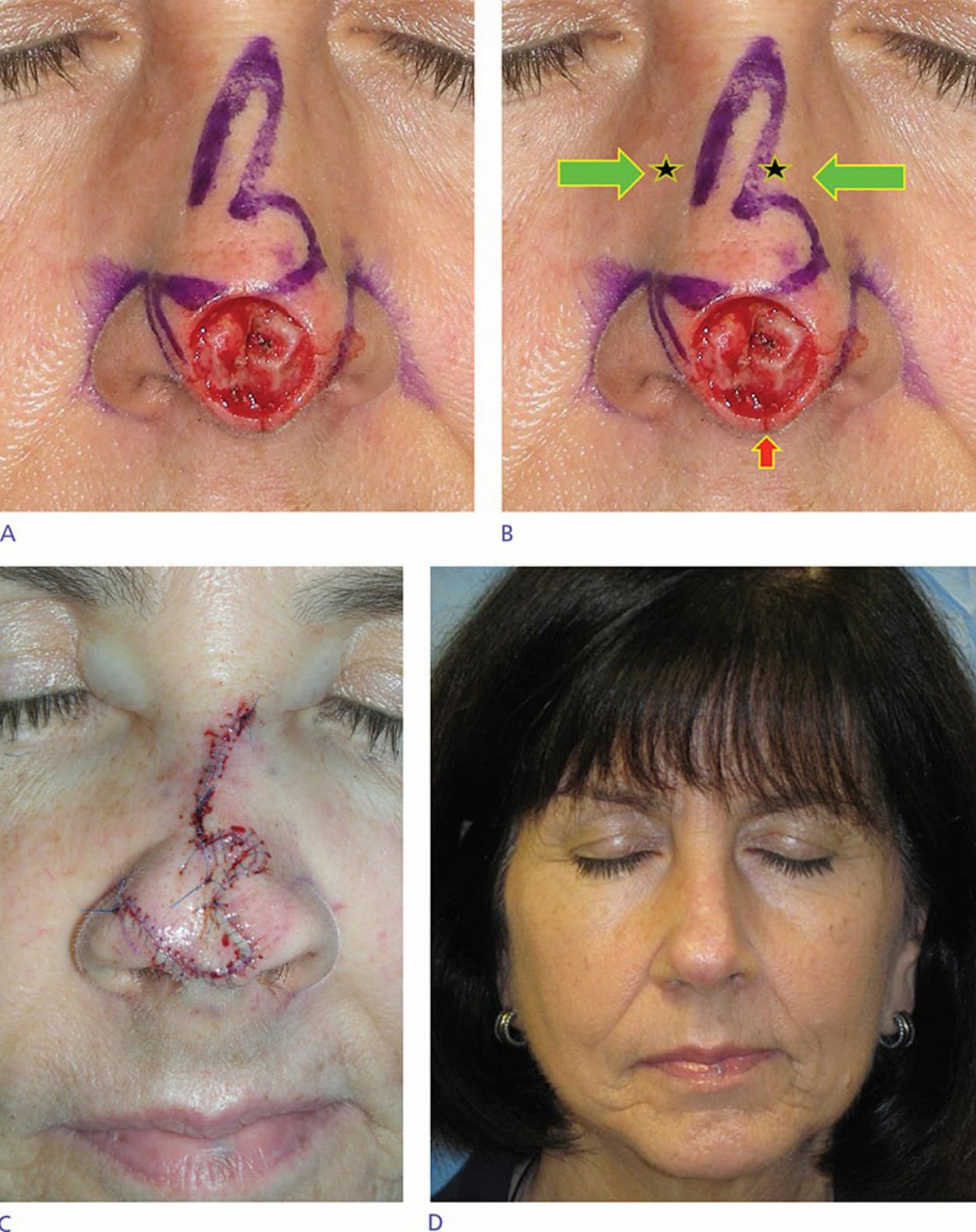
Figure 23-26 . Key design principles of a bilobed flap on the nose. (A) The diameter of the primary lobe is approximately equal to the diameter of the defect. The secondary lobe has a diameter 80% to 85% of the primary lobe and is not tapered too quickly. The standing cone is 30 degrees at the apex and oriented as vertically as possible without compromising the vascular pedicle. (B) Appropriately sized lobes minimize secondary motion at the nasal tip (red arrow). The final donor site is oriented such that the primary tension vector of its closure is parallel to the free margin (green arrows). (C) Immediate postoperative appearance. Note the absence of free-margin distortion. (D) Appearance at 8 months postoperatively after treatment with pulsed-dye laser.
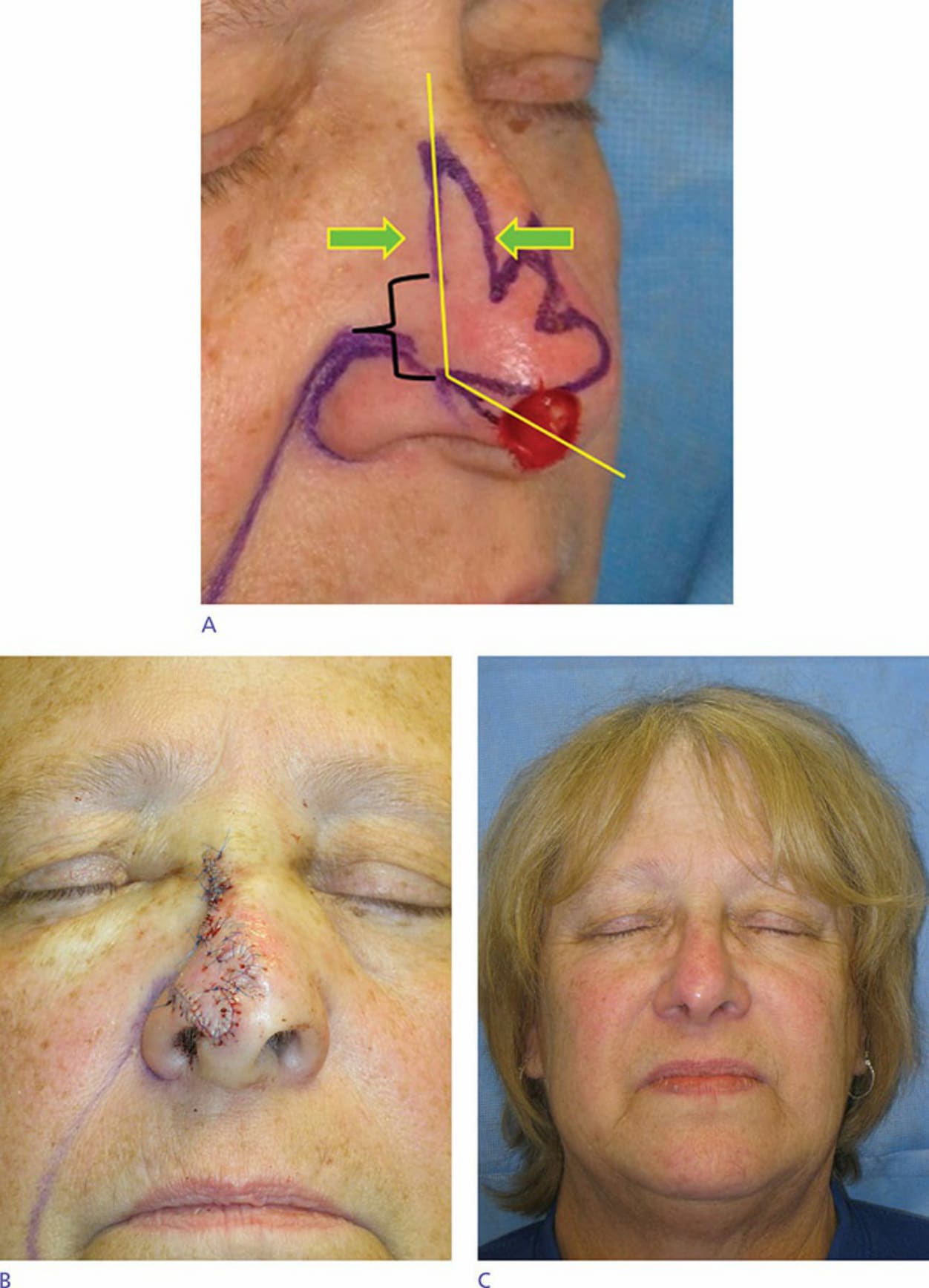
Figure 23-27. The trilobed flap has several design advantages. (A) The flap rotates 120 to 150 degrees, places the final defect in a more favorable location such that the key tension suture preserves the position of alar margins, and allows for a wide, more robust vascular pedicle. The trilobed flap also gains an additional Z-plasty advantage. (B) Immediate postoperative appearance. Note the preservation of alar symmetry. (C) Six-month follow-up.