Specific examples of single-lobed transposition flaps
Specific examples of single-lobed transposition flaps
Nasolabial transposition flap. The nasolabial single-lobed transposition flap is useful to reconstruct defects of the alar groove and ala, and is one of the most frequently performed banner flaps.3 The flap recruits tissue from the generous reservoir at the nasolabial fold. Since the alar groove and ala have scant fat, and since the skin adheres firmly to the dermal insertions of the underlying muscles, this flap can appear too thick and pincushion without a precise undermining plane and tacking sutures to recreate the alar groove.
The key design characteristics of the nasolabial transposition flap are shown in (Fig. 23-20). The medial arm of the flap takes from the lateral aspect of the nasal defect and extends inferiorly along the nasolabial fold. The lateral arm of the defect extends along the cheek in a parallel line that gently tapers to join the inferior nasolabial fold with 30 degrees or less. The horizontal widths of the proximal flap and defect should be identical. The superior aspect of the cheek limb of the flap should remain a couple of
millimeters inferior to the origination point of the medial limb. This slight discrepancy is important to orient the primary tension vector in a superomedial vector that recruits skin from the mobile buccal cheek.
The flap is elevated to include only the subdermal fat (Fig. 23-21A). If it includes the nasolabial fat pad, the flap will have too much volume. The nasolabial fold and cheek are undermined in the same tissue plane.
The key suture closes the donor defect at the flap’s origination point. If the wound is under high tension, tacking the cheek to the origin of the transverse nasalis along the pyriform aperture may be necessary to avoid lateral distraction of the nose (Fig. 23- 21B). The distal portion of the flap is trimmed to match the size of the defect, and it is sutured to the primary defect. The alar groove has a deep concavity and the flap will pincushion if the dead space is not closed. Tacking the base of the flap to the caudal margin of the transverse nasalis muscle is usually necessary to close dead space and restore contour of the concave alar groove (Fig. 23-21C). Transposition of the flap creates a standing cone along the nasal sidewall, which is removed while taking care to preserve the flap pedicle. Pincushion deformity of the transposed portion of the flap is the most common complication, which can be minimized by wide undermining of the recipient site in the perichondrial/periosteal plane, placement of tacking sutures on the
flap to the base of defect, and judicious thinning of the flap resulting in a concave surface when the flap is inset. The desired contour should be present immediately postoperatively (Fig. 23-21D).
Double rhombic flaps. Two rhombic flaps may be used to cover defects that are too large for a single flap. Different variations of this strategy have been described. One variant has opposing rhombic flaps from the opposite sides of the primary defect (Fig. 23-22).4,5 Another variant has two mirror image flaps on each side of the primary defect.6,7 Each flap has a Dufourmentel modification with an acute takeoff angle, and they share a standing cone deformity when they are transposed.
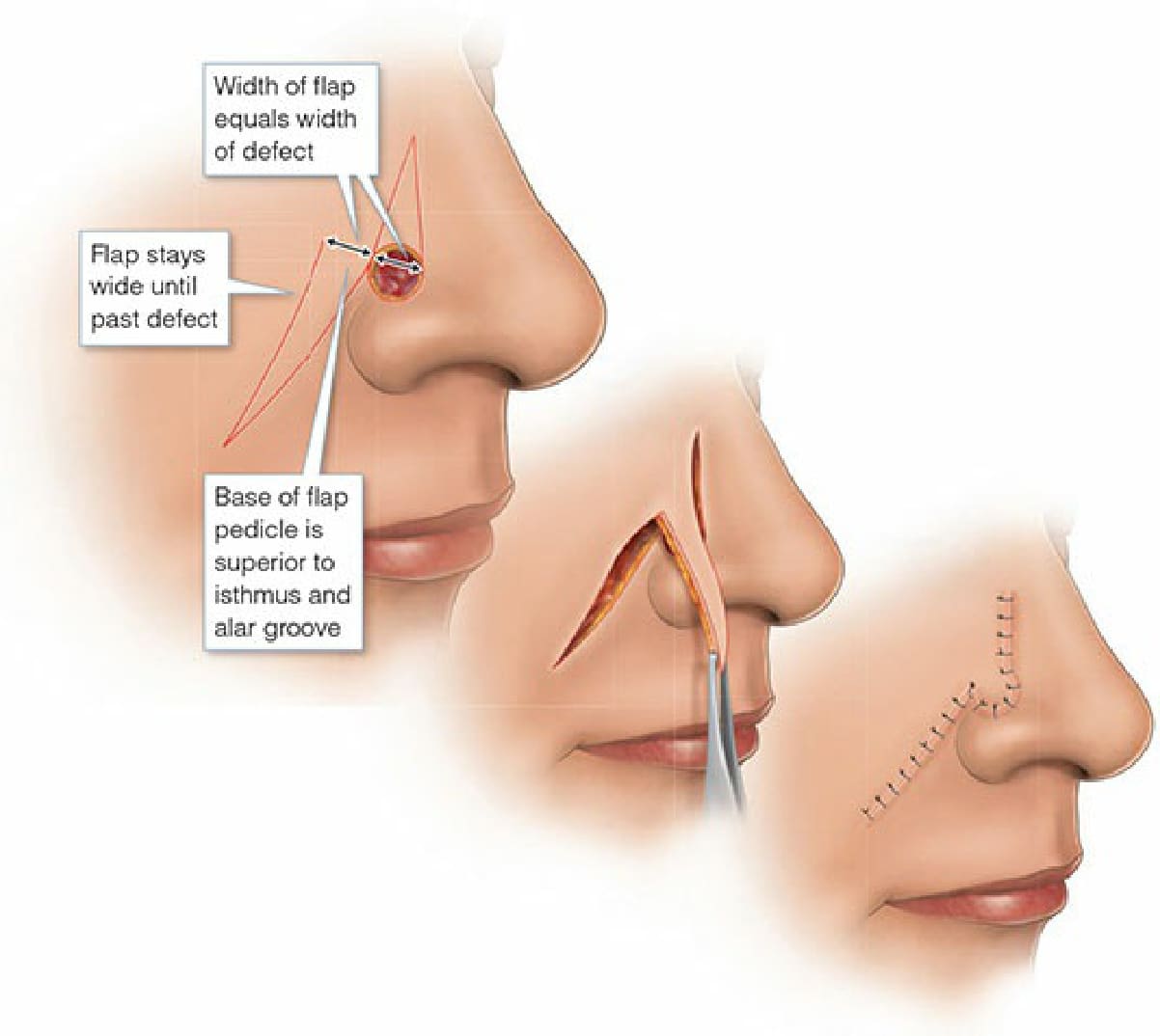
Figure 23-20. Design characteristics of the nasolabial transposition flap include equal widths of the flap and defect, maintaining the width of the flap until past the defect, and tapering the flap arms to an angle of 30 degrees or less.
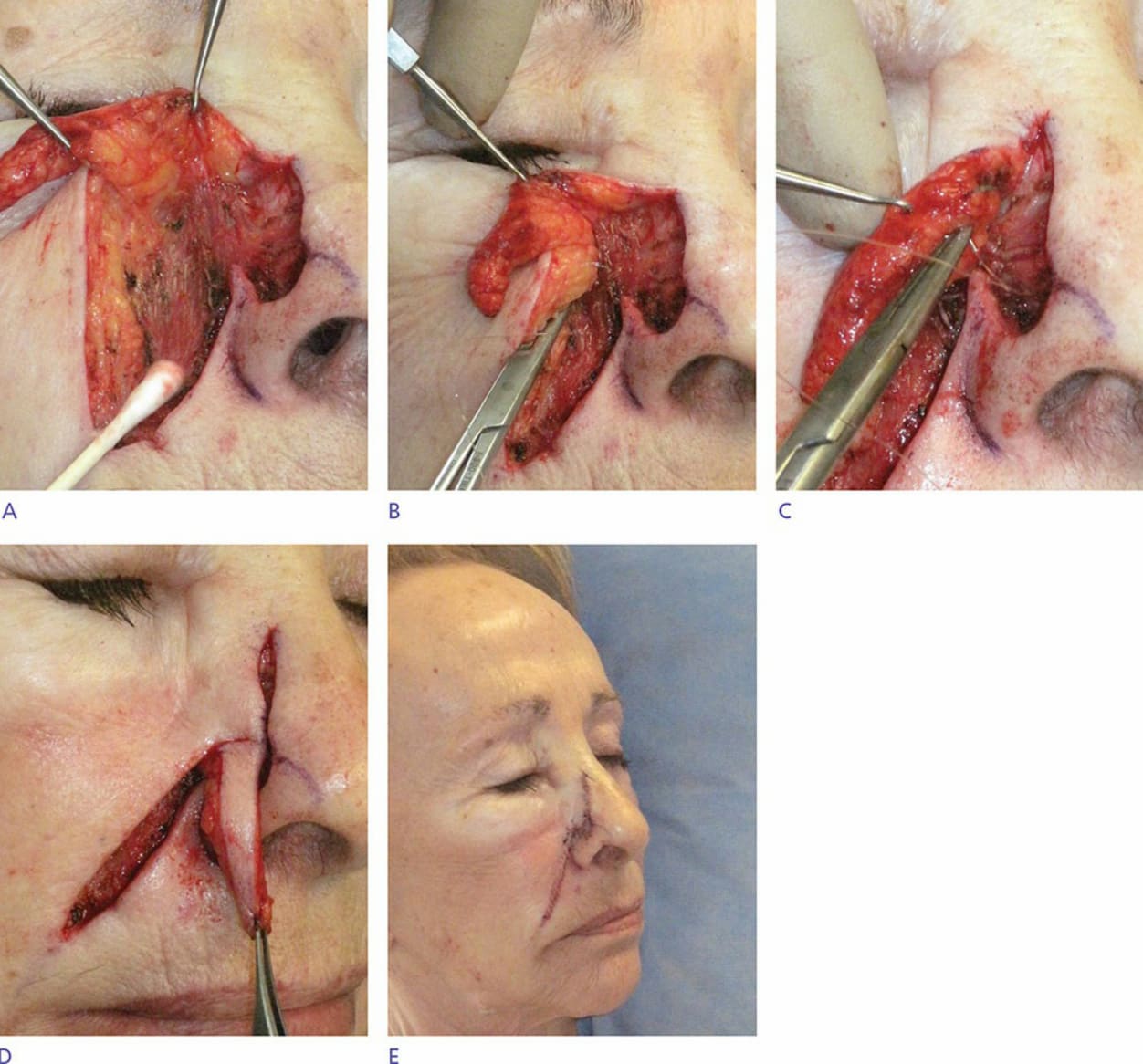
Figure 23-21. (A) Nasolabial transposition flap elevated under the subdermal fat and dissected off the lip elevators. Flaps that include the nasolabial fat pad will appear bulky. (B) Tacking the cheek to the pyriform aperture recreates the nasofacial sulcus and prevents distortion of the ala and tip. A slight dimple is desirable. (C,D) Tacking the base of the flap to the caudal margin of the transverse nasalis recreates the alar groove. A dimple is again desirable. (E) Desired contours should be evident immediately postoperatively.
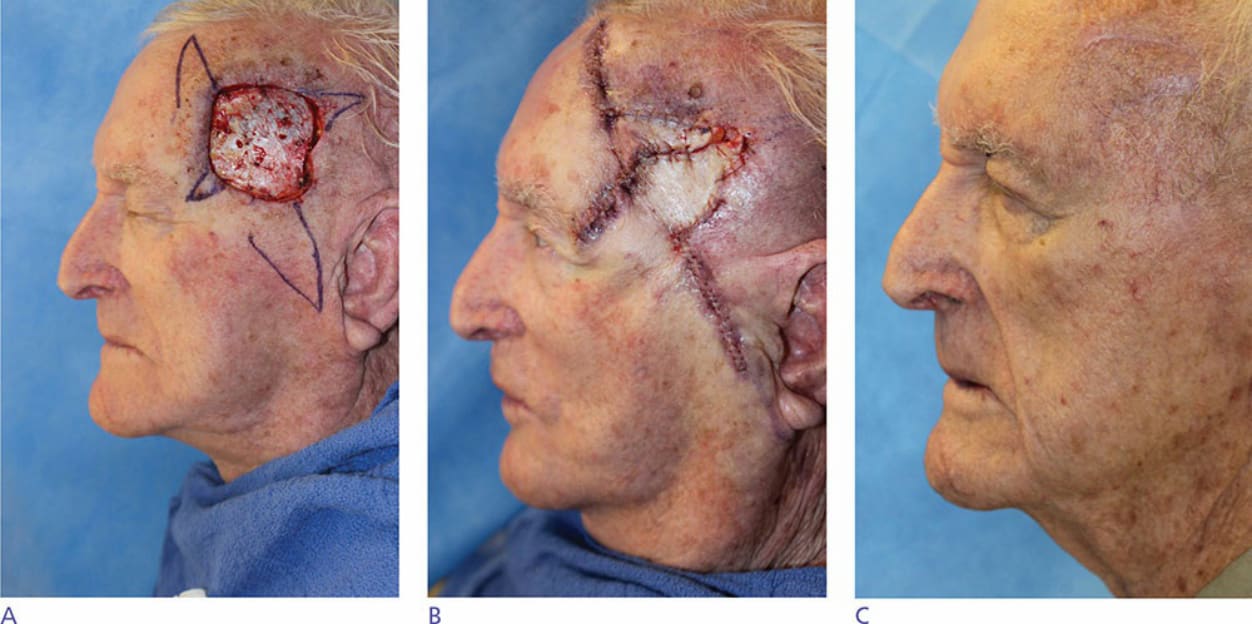
Figure 23-22 . Mohs defect on the temple repaired with opposing rhombic flaps. (A) Flap design. (B) Flaps sutured into place. (C) Three-month follow-up.