Tension on the flap
Tension on the flap
High tension on the flap increases the risk for ischemia. Common causes of tension include a flap with less surface area than the defect and transposition of the flap to a recipient bed with tight immobile skin. Transposition flaps on the scalp are particularly vulnerable to excessive tension.
Altering the defect or the flap to optimize flap design and execution
In order to maintain the appropriate contour of the recipient site, the primary defect is often deepened to match the flap thickness. For example, a shallow defect on the nasal tip may be deepened to perichondrium to match the thickness of a bilobed flap, which is elevated in the perichondrial plane. Additionally, the defect may be altered or enlarged to place scar lines along cosmetic subunit junctions. For instance, on the nasal ala, the defect may be extended to the alar rim to camouflage the horizontal scar line from a nasolabial transposition flap. Similarly, a defect on the lip may be extended to the vermilion–cutaneous junction (Fig. 23-15).
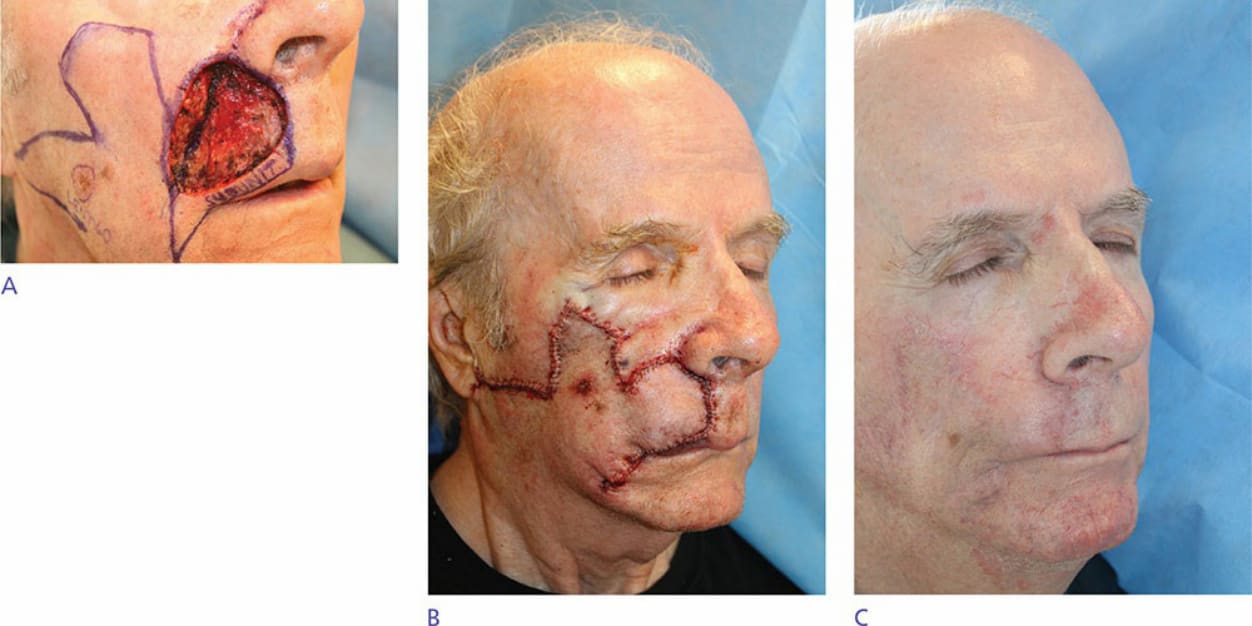
Figure 23-15. A defect on the upper lip is extended to the vermilion–cutaneous junction in order to camouflage the incision within the cosmetic subunit junction. Preoperative view and design (A), appearance immediately after closure (B) and appearance prior to revision to recreate the melolabial fold (C).